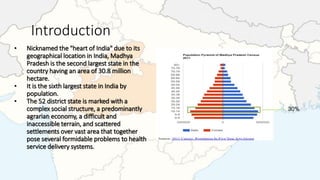

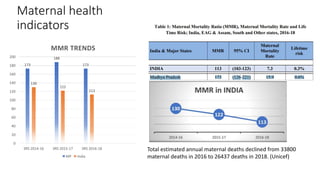
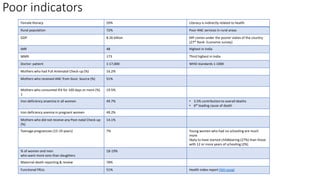
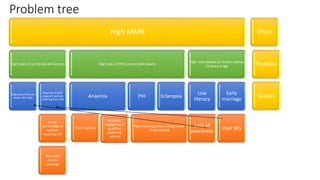
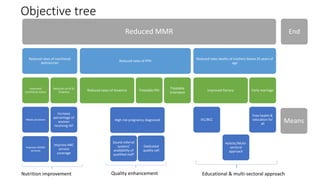



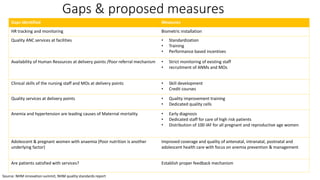



Madhya Pradesh has a high maternal mortality ratio of 173 deaths per 100,000 live births. Key contributing factors include low literacy, poor nutrition status of women, inadequate access to quality antenatal, delivery and postnatal care services, and high rates of anemia. While institutional deliveries have increased, many deliveries still occur at home without a skilled birth attendant. The proposed project aims to address these gaps by improving human resource tracking, standardizing and increasing the quality of antenatal services, ensuring availability of staff at delivery points, and strengthening the referral system.