Downloaded 112 times

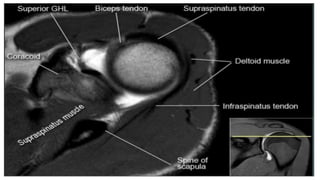
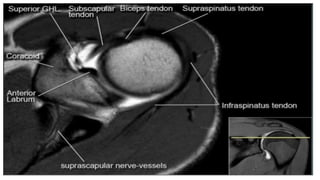
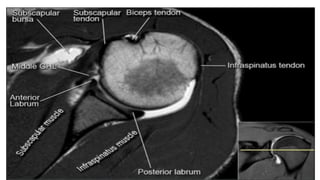
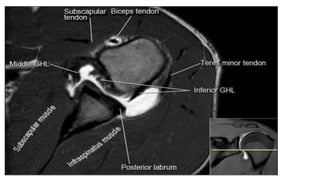
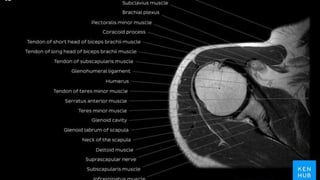
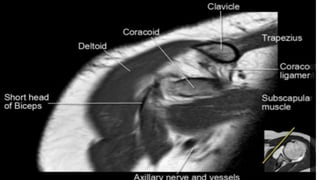

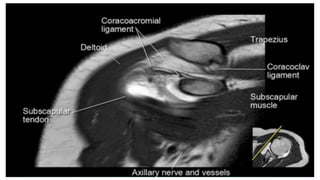
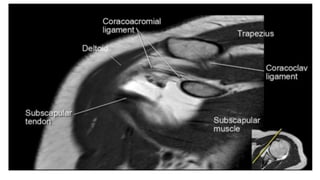
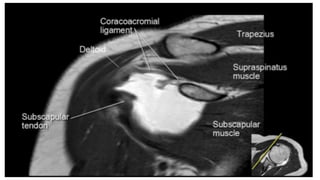
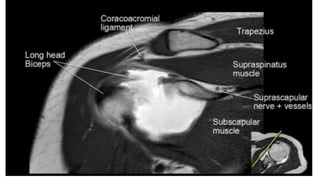
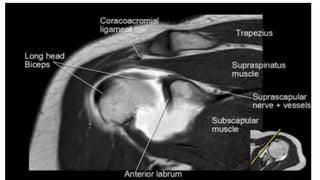
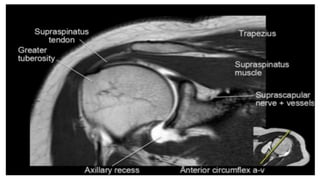


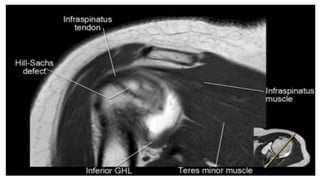

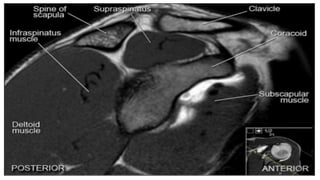
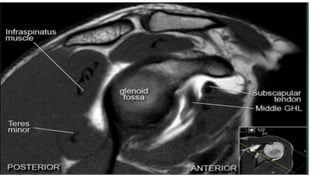
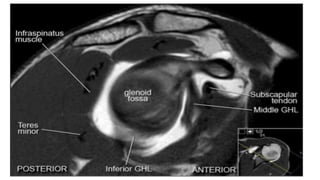
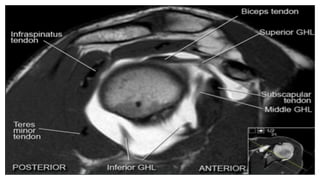
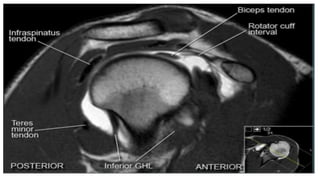
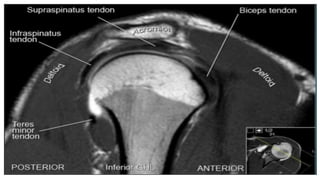

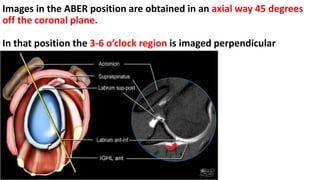
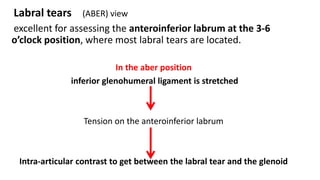
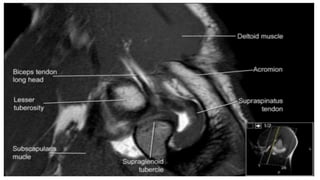


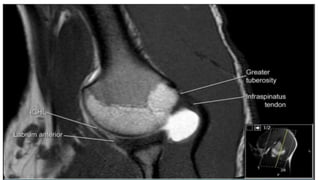
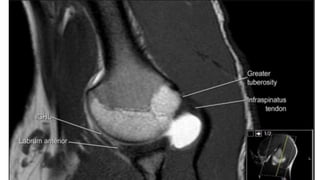
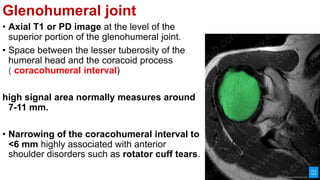
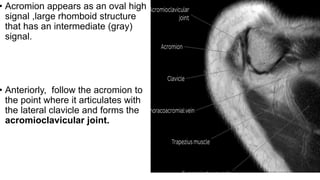

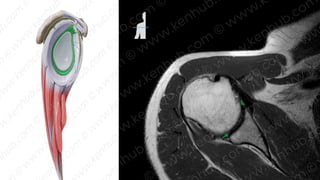
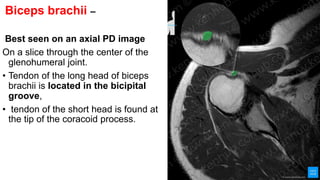
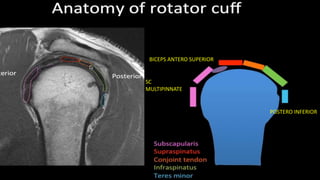
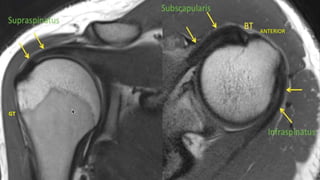
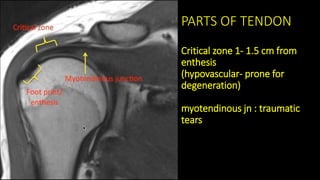
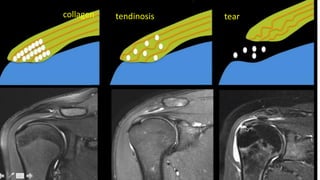



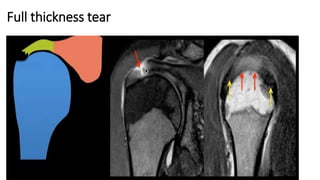
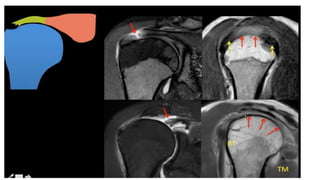
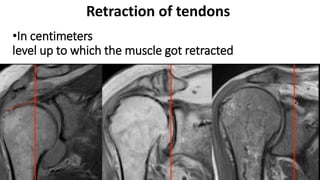

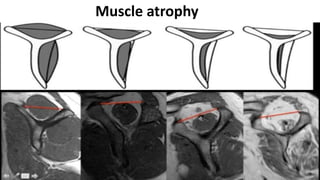




The document provides an overview of how to interpret shoulder MRI images, detailing the differences between T1 and T2 weighted images, as well as various imaging planes including coronal, sagittal, and axial. It covers key anatomical structures such as ligaments, labrum, and rotator cuff tendons, highlighting their appearances on MRI and the significance of certain measurements like the coracohumeral interval. Additionally, it explains the use of the aber view for assessing labral tears and the implications of certain findings in diagnosing shoulder disorders.


























![Femoroacetabular%20 impingement[1]](https://cdn.slidesharecdn.com/ss_thumbnails/femoroacetabular20impingement1-130422051258-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)








































