2. INTRODUCTION
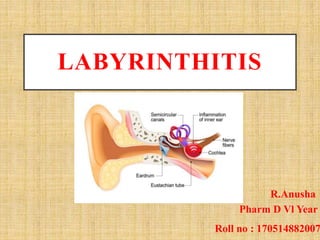
• Labyrinthitis- This is the inflammation of inner ear
(Cochlea) and / or balance organ (Utricle, Saccule
and Semicircular Canals) which are intimately
connected to each other inside the skull adjacent to
outer ear.
• It is the often a complication of infection of the
middle year(otitis media).
3. FUNCTION OF LABYRINTH
• The semi-circular canals sense movement of the head
and help to control balance and posture. The cochlea is
concerned with hearing.
• Head movements are sensed because when we move
our head, the fluid in the labyrinth within the semi-
circular canals moves too.
• The movement of the fluid moves tiny hairs on the
inside lining of the labyrinth.
• When the hairs move, this triggers nerve messages to be
sent to the brain via vestibular nerve.
4.
5. TYPES OF LABYRINTHITIS
There are three types of labyrinthitis:
Circumscribed
Thinning or erosion of bony capsule of labyrinth—
usually horizontal semicircular canal.
Diffuse serous
Diffuse intra labyrinthine inflammation without pus
formation.Reversible if treated early.
Diffuse suppurative
Diffuse pyogenic infection of the labyrinth
Permanent loss of vestibular and cochlear functions.
6. ETIOLOGY
• Viral or bacterial infections
• Cholesteatoma
• Drug toxicity(Aminoglycosides)
• Head injury
• Tumour
• Vasculitis
8. PATHOLOGY
• Infection usually occurs by one of three routes:
– From the meninges(Internal auditory canal,
Cochlear aqueduct or both)
– From the middle ear space
– Hematogenous spread
9. INVESTIGATION
Based on symptoms, medical history and physical
examination.
• Vestibular Testing
• Audiography
• CT(to rule out meningitis) and MRI ( to rule out
acoustic neuroma, stroke, brain abscess, or
epidural hematoma)
11. Anti histamines:These have antiemetic, anticholinergic and
antihistaminic properties.
It reduces the sensitivity of labyrinthine apparatus.
• Meclizine:
Vertigo: 25 – 100 mg daily in divided doses used as needed for
2-3 days.
• Dimenhydrate:
Vertigo: 25-50 mg PO Q8H
12. Phenothiazine derivatives: Antidopaminergic drugs that
can depress reticular activating system(this effect may be
responsible for relief of nausea and vomiting)
• Promethazine:
Nausea and vomiting: 25 mg TID
• Prochlorperazine:
Nausea and vomiting: 5 mg TID
13. • Viral labyrinthitis:
A short course of oral corticosteroids may be helpful in
reducing labyrinthine inflammation and prevent the
sequelae of labyrinthitis due to infectious or
inflammatory causes.
Currently, the role of antiviral therapy is not established.
• Bacterial labyrinthitis:
Antibiotic treatment is based on culture and sensitivity.
Antibiotic treatment should consist of broad spectrum
antibiotic or combination therapy with CNS penetration
until culture results are available.
14. • Surgical treatment:
Mastoid exploration is often required in chronic otitis
media and cholesteatoma.
Cortical mastoidectomy for control of suppurative
otitis media or
Radical mastoidectomy and labyrinthitis with dead
labyrinth to prevent intracranial extension of infection.
Surgical excision of cholesteatoma
Incision and drainage
Labyrinthectomy
15. REFERENCES
• https://studylib.net Ear infections
• Diseases of Ear, Nose and Throat and head
and neck surgery, PL Dhingra, S Dhingra.
6th edition
• Medscape