
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Zollinger Ellison Syndrome: Causes, Symptoms and Treatment
Similar to Zollinger Ellison Syndrome: Causes, Symptoms and Treatment (20)
More from Anusha Rameshwaram
More from Anusha Rameshwaram (20)
Recently uploaded
Recently uploaded (20)
Zollinger Ellison Syndrome: Causes, Symptoms and Treatment
- 1. ZOLLINGER ELLISON SYNDROME R.Anusha Pharm D Vl Year Roll no : 170514882007
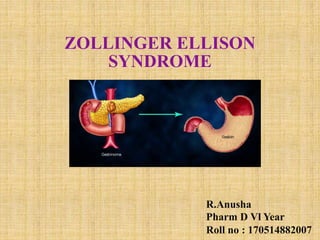
- 2. DEFINITION Zollinger-Ellison syndrome is due to gastrin- secreting tumors called Gastrinomas which may be duodenal or pancreatic endocrine tumors. Non-beta cells of the pancreatic tumor produce a large amount of gastrin and patients suffer from ulcers. • Gastrin level is highly increased. • The gastrin leads to increased production of the acid and there is a high level of HCL which leads to multiple ulcers in the stomach and small bowel. Gastrinoma may occur in the stomach, pancreas, lymph nodes mesentery.
- 4. PATHOPHYSIOLOGY Gastrin is a potent hormone for the secretion of gastrin from gastric G cells, Proximal duodenal G cells, and pancreatic delta cells. This is under the control of vagal stimulation. Gastrin production: o Endocrine cells (G cell) of the antral mucosa of the stomach. o The lesser amount of the G cells of proximal duodenum. o A small amount from delta cells in the pancreas.
- 6. Gastrin is secreted in response to : Antral distension. Meals. Partially digested food (Proteins). Free amino acids also stimulate gastrin. Carbohydrates and Fats have little effect on gastrin secretion. Other gastrin release stimulants are: Alcohol. Caffeine. Insulin-induced hypoglycemia. Calcium ingestion or I/V infusion. Vagal stimulation by:Smell,Tasting,Swallowing,Chewing.
- 7. Increased fasting gastrin level is associated with increasing age over 60 years. Secretion of gastrin depends upon the pH of gastric acid (HCl): pH 5 to 7: Gastrin secretion is maximum. pH 2.5: Gastrin secretion is reduced by 80%. pH 1.0: Maximum suppression of Gastrin production.
- 8. •Most gastrinomas arise in the duodenum. •Gastrinomas located in the pancreas carry a greater malignant potential. •Around 25% of the patient with gastrinoma have multiple tumors as a part of a condition called Multiple endocrine neoplasia types 1 (MEN-1) MEN 1 has the tumors in the pituitary gland, and parathyroid gland in addition to the tumor of the pancreas.
- 10. Diagnosis of Gastrinoma Raised level of Gastrin (Hypergastrinemia). Fasting gastrin level is markedly raised from 2 to 2000 times normal. Gastrin level of 1000 ng/L (ng/L; greater than 481 pmol/L) is diagnostic and the basal acid output (BAO) is more than or equal to 15 mEq/h (more than or equal to 15 mmol/h).
- 11. Normal gastrin levels: Fasting level-up to 100 ng/L. Older people over 60 years = 100 to 800 ng/L. Adult = 0 to 180 ng/L. Child = 0 to 125 ng/L. The level fluctuates during the day: Highest during the daytime. After the meal. The lowest level from 3.00 to 7.00 am.
- 12. TREATMENT •PPIs are now the drugs of choice for treating gastric acid hypersecretion in patients with ZES because of their long duration of action and potency. •Many of the PPIs (omperazole, esomeprazole, lansoprazole, esomeprazole, rabeprazole, and pantoprazole) are effective in ZES. •Initial doses of 80 mg/day for pantoprazole (or an equivalent dose of other available PPIs) given every 8 to 12 hours is most effective at controlling gastric acid hypersecretion and reliving symptoms. IV PPIs can be used for those patients who do not tolerate oral therapy.
- 13. •PPIs must be dose adjusted in patients with ZES to normalize BAO levels to less than 15 mEq/h (less than 15 mmol/h) or less than 5 mEq/h (5 mmol/h) in patients with reflux esophagitis or prior operations to reduce acid secretion, such as subtotal gastrectomy. •PPI therapy can be gradually decreased after adequate control of hypersecretion is achieved. •Since 60% to 90% of gastrinomas are malignant, management of advanced disease may include surgical resection of primary and metastatic gastrinomas. •Nonsurgical therapy may include treatment with chemotherapy, somatostatin analogues such as octreotide, interferon, and targeted-molecular therapies such as a mTor inhibitor (everolimus) or a tyrosine-kinase inhibitor (sunitinib).
- 14. •Octreotide inhibits gastric acid secretion and lowers serum gastrin levels, its subcutaneous route of administration and side effects make it less desirable in therapeutic setting. •For ZES patients with MEN1,parathyroidectomy should be considered because correction of hyper parathyroidism often reduces serum calcium levels and lowers gastrin secretion and acid out put. •Patients with metastatic gastrinomas can be treated with chemotherapeutic agents to inhibit the growth of these tumours.Such chemotherapy is generally streptozocin based,and involves using a combination of streptozocin,5 fluoracil and doxorubicin. • Targeted therapy Everolimus and Sunitinib can be used for advanced tumours.
- 15. REFERENCE Joseph T Dipiro; Pharmacotherapy: A Pathophysiologic Approach;10 edition, Zollinger-Ellison Syndrome; Pg :1531-1533. Labpedia.net (Zollinger Ellison Syndrome). Zollinger Ellison Syndrome-NORD National organisation for rare diseases.
Editor's Notes
- Vagal efferents release acetyl choline , which acts on M3 receptors that are present on parietal cells, resulting in increased acid production.
- Large doses of insulin(.2.5 U/kg) causes marked hypergastrinemia by the release of histamine which is the kost important positive regulation mechanism of the secretion of gastric acid in the stomach. 12mg/kg of calcium gluconate over 3 hours causes the gastrin level to more than double in patients with gastrinoma. Activation of the calcium sensing receptors on the basal and apical surfaces of human G cells located in the antrum of the stomach stimulates gastrin and gastric acid secretion.