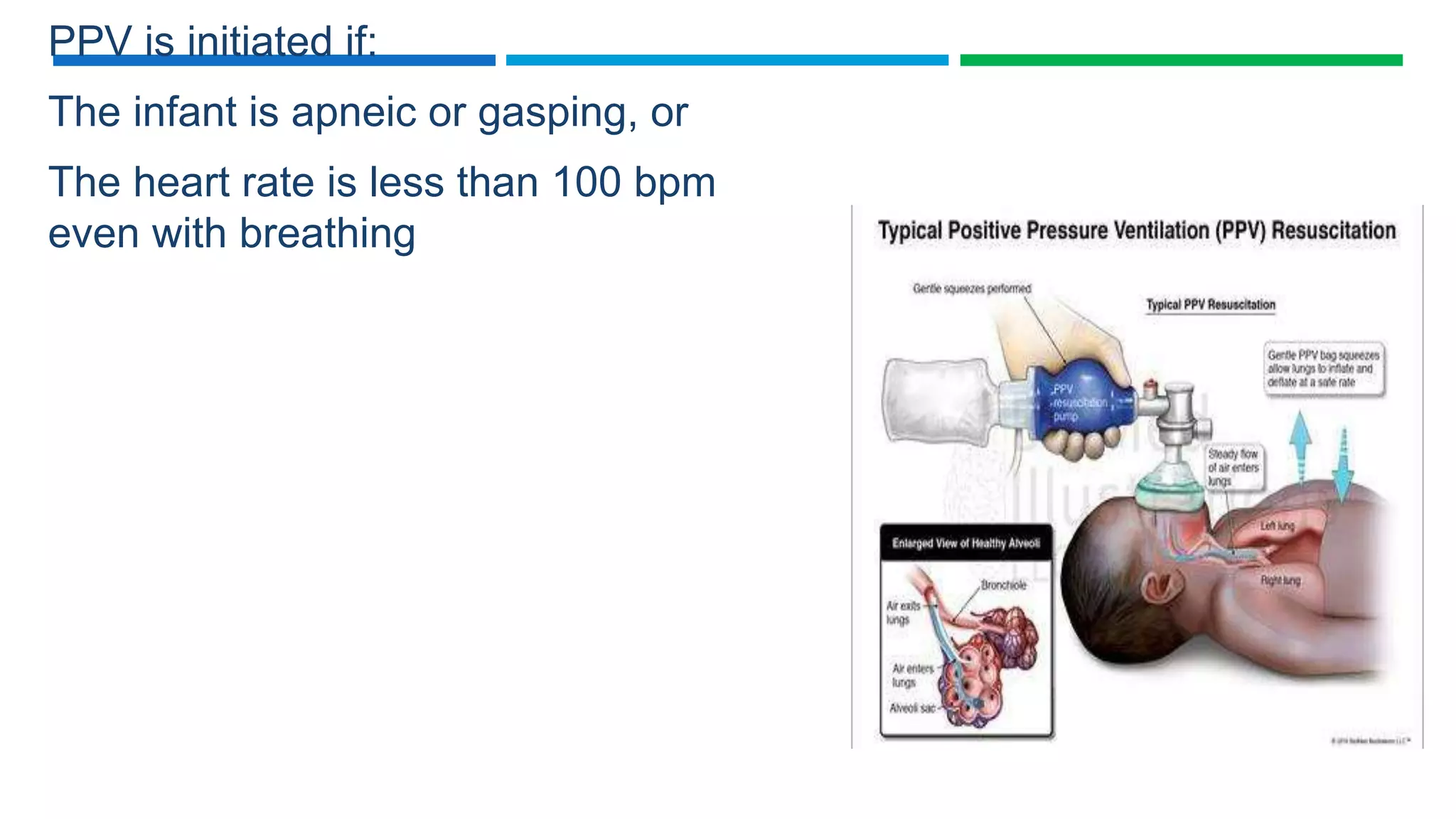
This document provides an overview of neonatal resuscitation. It begins with introductions stating that 10% of newborns require some form of resuscitation. It then discusses the importance of resuscitation, risks for breathing problems, and key steps for successful resuscitation including being prepared, knowing procedures, and documentation. The document outlines the initial steps of resuscitation including drying, positioning, clearing airways, and providing tactile stimulation. It provides details on evaluating the need for further resuscitation and describes providing routine care for crying babies or beginning further resuscitation steps if the baby is not crying.






































































































![NEONATAL RESUSCITATION [Autosaved] 2018.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved2018-250921081223-1a2be906-thumbnail.jpg?width=640&height=640&fit=bounds)







![Neonatal resuscitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved-210325082037-thumbnail.jpg?width=640&height=640&fit=bounds)


























