Nephrotic syndrome
•
9 likes•3,001 views

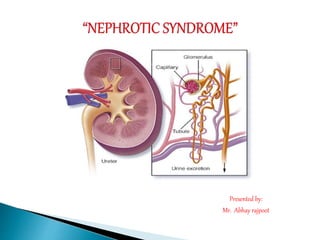
–The syndrome is apparent in any condition that seriously damage the glomerular capillary membrane that results in increase glomerular capillary permeability to plasma proteins. Although liver is capable of increasing the production of protein. It can’t keep up with the daily loss of albumin through the kidney. Thus hypoalbuminemia results.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Nephrotic syndrome
Similar to Nephrotic syndrome (20)
More from Abhay Rajpoot
More from Abhay Rajpoot (20)
Recently uploaded
Recently uploaded (20)
Nephrotic syndrome
- 1. Presented by: Mr. Abhay rajpoot
- 2. The syndrome is apparent in any condition that seriously damage the glomerular capillary membrane that results in increase glomerular capillary permeability to plasma proteins. Although liver is capable of increasing the production of protein. It can’t keep up with the daily loss of albumin through the kidney. Thus hypoalbuminemia results.
- 3. Nephrotic syndrome is a collection of symptoms due to kidney damage. This includes protein in the urine, low blood albumin levels, high blood lipids, and significant swelling.
- 4. Nephrotic syndrome is quite rare but has an important role to play in the development of kidney disease. In adults, the incidence of the condition is approximately 3 cases per 100,000 per year. The incidence of minimal change disease in Caucasian children is reported to be 2 per 100,000.
- 5. Medical conditions that can damage the kidneys Certain medications. Certain infections.
- 6. Nephrotic syndrome is usually caused by damage to the clusters of tiny blood vessels (glomeruli) of the kidneys.
- 7. Auto immune reaction Diabetic kidney disease. Minimal change disease Renal disorder Membranous nephropathy. Systemic lupus erythematosus Blood clot in a kidney vein.
- 9. Proteinuria Hypoalbuminemia Edema – Periorbital edema, pitting edema, ankle edema, Ascites, pleural effusion, Weight gain, hypertension Fatigue, headache, malaise and irritability Foamy appearance of urine (decrease surface tension by severe proteinuria) Haematuria Thrombophilia (clot formation) Lipiduria Dyspnoea Anaemia
- 12. .
- 13. Blood clots High blood cholesterol and elevated blood triglycerides Poor nutrition High blood pressure Acute kidney failure Chronic kidney disease Infections
- 14. Cholesterol-reducing medications. Medications called statins can help lower cholesterol levels. Ex. -Atorvastatin -Fluvastatin
- 15. Blood thinners. Medications called anticoagulants help decrease blood's ability to clot. Ex. -Heparin -Warfarin
- 16. Immune system-suppressing medications. Medications to control the immune system, such as – Ex. -Corticosteroids
- 17. Nursing Assessment Edema. Observe for edema when performing physical examination of the child with nephrotic syndrome. Weight and measure. Weight the child and record the abdominal measurements to serve as a baseline. Vital signs. Obtain vital signs, including blood pressure. Pitting edema. Note any swelling about the eyes or the ankles and other dependent parts. Skin. Inspect the skin for pallor, irritation, or breakdown; examine the scrotal area of the male child for swelling, redness, and irritation.
- 18. 1) Nursing diagnosis – excessive fluid volume related to damage glomeruli as evidence by I/O chart, edema and weight gain. Nursing goal – To maintain fluid volume Intervention – Assess fluid status, Monitor I/O ratio. Limit fluid and sodium intake to prescribed volume. Explain to patient and family rational for fluid resuscitation. Oral hygiene is to be encouraged. To provide the diuretics
- 19. 2) Nursing diagnosis – risk of infection related to edema & altered immune response as evidence by weight gain, I/O chart, taking temperature. Nursing goal – To prevent from infection Intervention- Limited fluid intake Provide meticulous skin care To monitor I/O chart. To check daily weight. To check the TPR. Use strict aseptic technique To provide the diuretics and antipyretics.
- 20. 3) Nursing diagnosis – Disturbed thought process related to effect of uremic toxin on CNS as evidence by confusion, LOC, impair ability to process external stimuli. Nursing goal – To stabilize the thought process Intervention – Assess the extent of impairment in thought process. Orient to time, place and person. To provide diuretic, antibiotics to the patient. Preserving neurological functioning. Use seizure precaution. Encourage the patient to turn & in any type of activity as due to drowsiness and lethargy. Give psychological support. Prepare for hemodialysis
- 21. Goals are met as evidenced by: Relief from edema. Improvement of nutritional status. Maintenance of skin integrity. Conservation of energy. Prevention of infection.
- 22. Chlorambucil, in combination with prednisone, was compared with prednisone alone in a randomized controlled trial in 21 children to assess its effect on the duration of remission (improvement) and the rate of relapse (deterioration after improvement). All control patients treated with prednisone alone continued to relapse at the same rate, with all patients experiencing a return of proteinuria by seven months. Conversely, those who received the same prednisone therapy along with chlorambucil for six to 12 weeks remained in complete remission, without further medication, during 12 to 34 months of follow-up observation.
- 23. https://emedicine.medscape.com/article/244631- overview https://en.wikipedia.org/wiki/Nephrotic_syndrome https://www.mayoclinic.org/diseases- conditions/nephrotic-syndrome/symptoms- causes/syc-20375608 http://www.renalmed.co.uk/database/nephrotic- syndrome http://www.kidneyfund.org/kidney-disease/other- kidney-conditions/nephrotic-syndrome.html https://nurseslabs.com/nephrotic-syndrome/