Downloaded 613 times





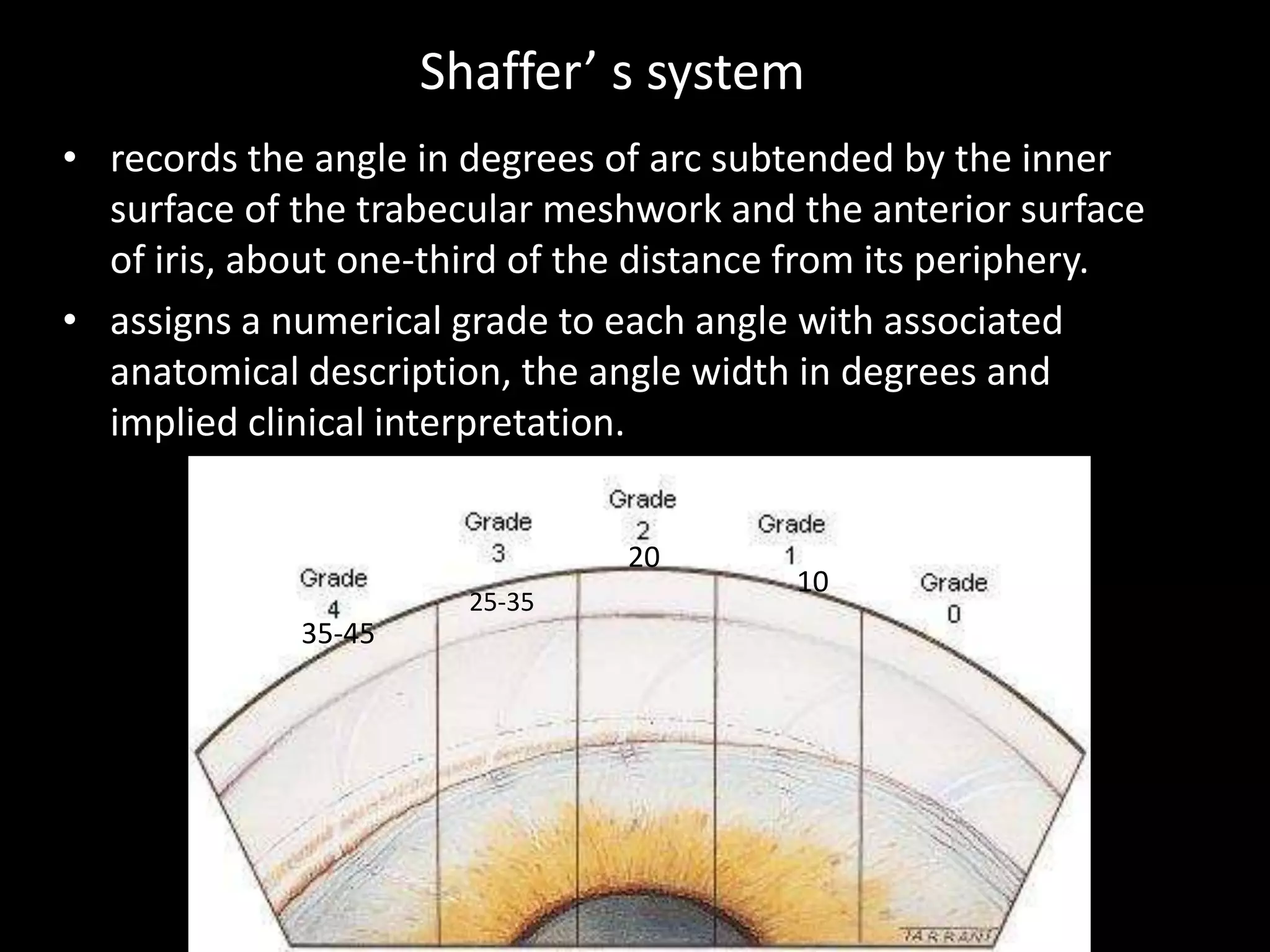
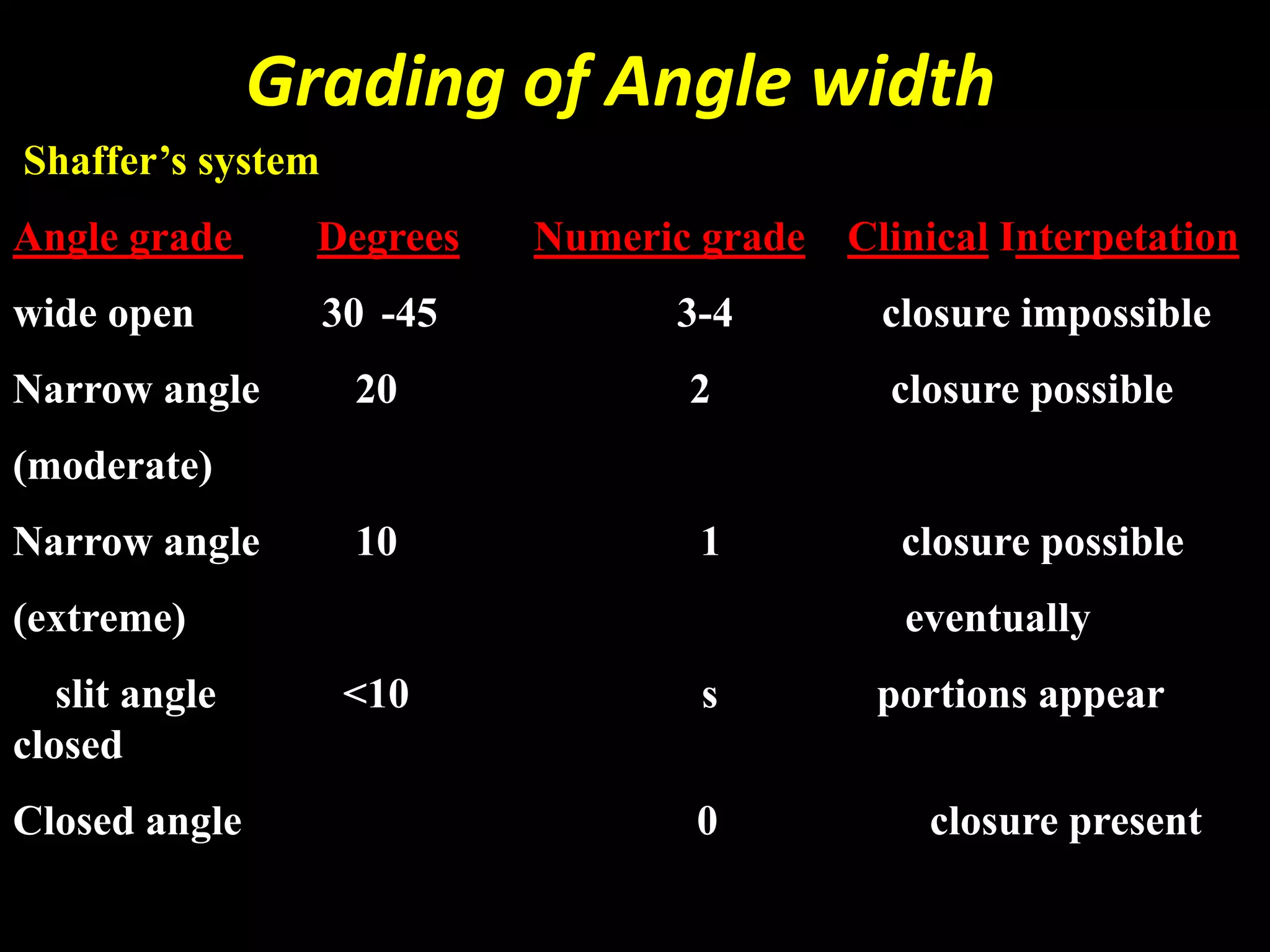
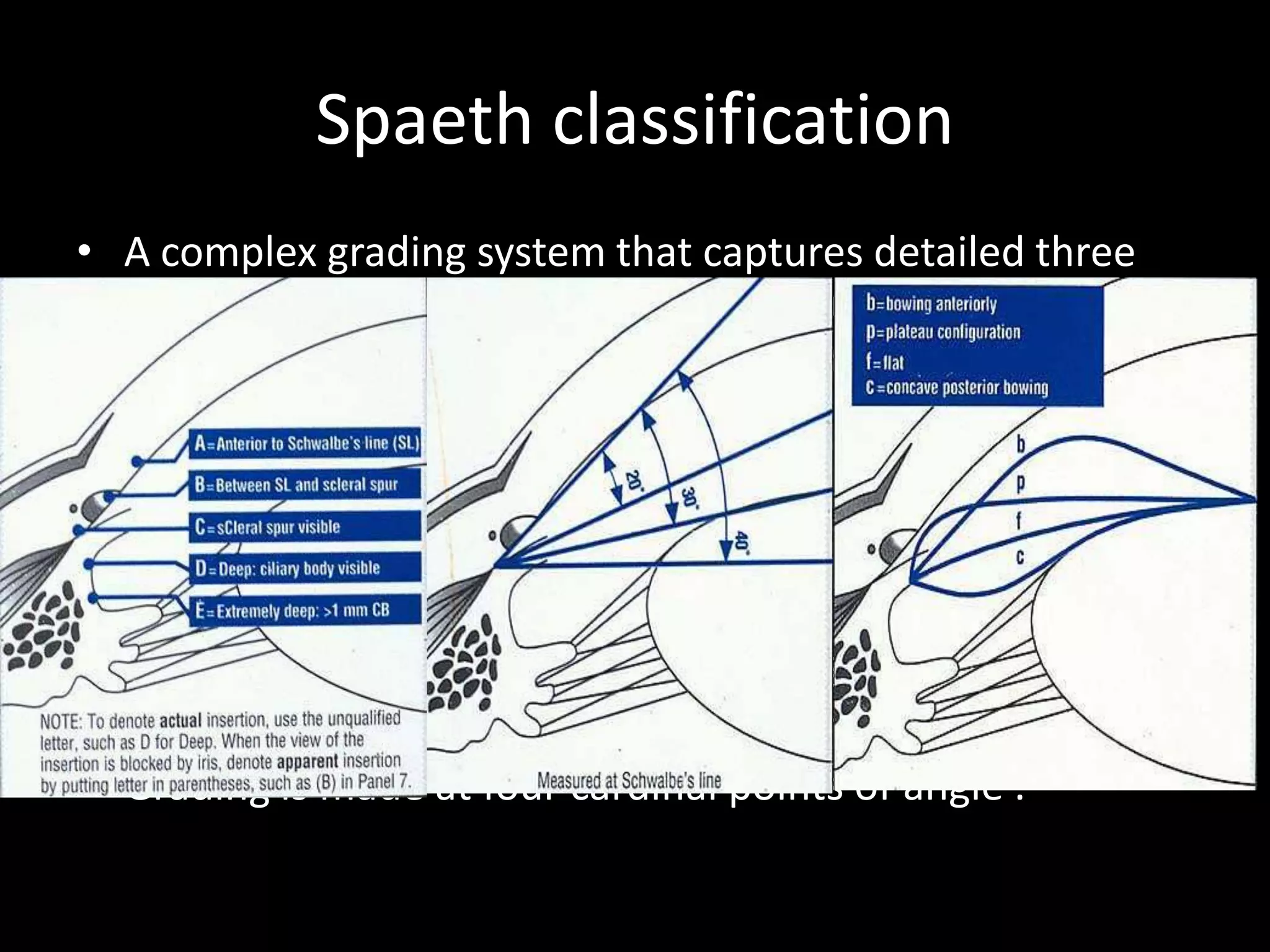

The document provides a comprehensive overview of gonioscopy, a crucial technique in ophthalmology for assessing the anterior chamber angle and diagnosing conditions like glaucoma. It details the anatomy of the angle, techniques for direct and indirect gonioscopy, grading systems such as the Shaffer and Spaeth systems, and identifies various abnormalities. The text emphasizes the importance of routine gonioscopy for preventing glaucoma-related blindness and the advancements in goniolens technology.



































































