Rheumatic heart disease: Acute Rheumatic Fever
•Download as PPTX, PDF•
98 likes•13,954 views

Rheumatic heart disease: Acute Rheumatic Fever

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Rheumatic heart disease: Acute Rheumatic Fever
Similar to Rheumatic heart disease: Acute Rheumatic Fever (20)
More from Pratap Tiwari
More from Pratap Tiwari (20)
Recently uploaded
Recently uploaded (20)
Rheumatic heart disease: Acute Rheumatic Fever
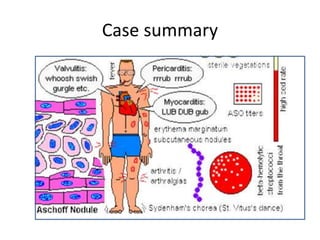
- 1. Case summary
- 2. Rheumatic heart disease: Acute rheumatic fever Pratap Sagar Tiwari
- 3. Introduction :ARF • RF is an acute, immunologically mediated, multisystem inflammatory disease involving heart, joints, CNS, skin and other tissues that occurs a few wks (2-4 Wks) after an episode of group A β-hemolytic streptococcal pharyngitis. • RHD is the cardiac manifestation of RF and is a/w inflammation of the valves, myocardium, or pericardium. • ARF usually affects children (MC betwn 5-15 yrs)
- 4. Pathophysiology • The condition is triggered by an immune-mediated response to infection with specific strains of group A streptococci, which have antigens that may cross-react with cardiac myosin and sarcolemmal membrane protein. • Antibodies produced against the streptococcal antigens cause inflammation in the endocardium, myocardium and pericardium, as well as the joints and skin.
- 5. Histology • Aschoff nodules are pathognomonic and occur only in the heart. • They are composed of multinucleated giant cells surrounded by macrophages and T lymphocytes. • Are not seen until the subacute or chronic phases of rheumatic carditis. • Anitschkow cells are enlarged macrophages found within granulomas (called Aschoff bodies).
- 6. The Jones Criteria Major Minor Migratory arthritis (predominantly involving the large joints) Carditis and valvulitis (eg, pancarditis) Sydenham chorea Erythema marginatum Subcutaneous nodules • Fever, Arthralgia • Elevated acute phase reactants [(ESR), (CRP)] • Prolonged PR interval The probability of acute rheumatic fever is high in the setting of group A streptococcal infection followed by two major manifestations or one major and two minor manifestations .
- 7. Evidence of Streptococcal pharyngitis • Positive throat culture for group A beta-hemolytic streptococci • Positive rapid streptococcal antigen test • Elevated or rising antistreptolysin O antibody titer.
- 8. There are 3 circumstances in which a presumptive DX of ARF can be made without strict adherence to the above criteria : • Chorea as the only manifestation. • Indolent carditis . • Recurrent rheumatic fever in patients with a history of rheumatic fever or rheumatic heart disease.
- 9. Pharyngitis: GAS infection vs Viral Infection F s/o GAS infection F s/o Viral Infection Patient 5 to 15 years of age Conjunctivitis Fever, Headache Coryza Sudden onset of sore throat Cough Beefy, swollen, red uvula Diarrhea Pain with swallowing Hoarseness Nausea, vomiting, abdominal pain Tender, enlarged anterior cervical nodes Scarlet fever rash Soft palate petechiae (doughnut lesions”) Tonsillopharyngeal erythema,exudates Adapted from Gerber MA, Baltimore RS, Eaton CB, et al. endorsed by the American Academy of Pediatrics. Circulation. 2009;119(11):1543.
- 10. Carditis :50-60% • A 'pancarditis' involves the endocardium, myocardium and pericardium to varying degrees. • May manifest as breathlessness (due to HF or p.effusion), palpitations or chest pain (usually due to pericarditis or pancarditis). • Other: tachycardia, cardiac enlargement and new or changed cardiac murmurs. • A soft systolic murmur due to MR is very common. A MDM (the Carey Coombs murmur) is typically due to valvulitis, with nodules forming on the MV leaflets. • AR occurs in about 50% but TV and PV are rarely involved. • Pericarditis may cause chest pain, a pericardial friction rub.
- 11. Arthritis :60-75% • MC major manifestation and tends to occur early when streptococcal antibody titres are high. • An acute painful asymmetric and migratory inflammation of the large joints typically affects the knees, ankles, elbows and wrists. • The joints are involved in quick succession and are usually red, swollen & tender for btn a day and 4 wks. • The pain characteristically responds to aspirin; if not, the diagnosis is in doubt.
- 12. Skin lesions: <5 % • Erythema marginatum :The lesions start as red macules (blotches) that fade in the centre but remain red at the edges and occur mainly on the trunk and proximal extremities but not the face. • Subcutaneous nodules :They are small (0.5-2.0 cm), firm and painless, non pruritic and are best felt over extensor surfaces of bone or tendons. They typically appear more than 3 weeks after the onset of other manifestations .
- 13. Erythema marginatum / Subcutanous nodules http://www.hxbenefit.com/erythema-marginatum.htm http://www.doctortipster.com/1789-rheumatic-fever.html l
- 14. Sydenham's chorea 2-30 % • This is a late neurological manifestation that appears at least 3-8 months after the episode of ARF, when all the other signs may have disappeared. • It occurs in up to 1/3rd of cases and is more common in females. • Emotional lability may be the first feature and is typically followed by purposeless involuntary choreiform movements of the hands, feet or face. Speech may be explosive and halting. • Spontaneous recovery usually occurs within a few months. • Approximately one-quarter of affected patients will go on to develop chronic rheumatic valve disease.
- 15. Primary Prevention of Rheumatic Fever (Treatment of Streptococcal Tonsillopharyngitis)
- 16. AHA Recommendations for Duration of Secondary Prophylaxis Category of Patient Duration of Prophylaxis RF without carditis For 5 years after the last attack or 21 years of age (whichever is longer) RF with carditis but no residual valvular disease For 10 years after the last attack, or 21 years of age (whichever is longer) RF with persistent valvular disease, evident clinically or on echocardiography For 10 years after the last attack, or 40 years of age (whichever is longer). Sometimes lifelong prophylaxis.
- 17. Chronic rheumatic heart disease • Chronic VHD develops in at least half of those affected by rheumatic fever with carditis. Two-thirds of cases occur in women. • The mitral valve is affected in more than 90% of cases; the aortic valve is the next most frequently affected, followed by the tricuspid and then the pulmonary valve. • Isolated MS accounts for about 25% and an additional 40% have mixed MS/MR.
- 18. Poststreptococcal reactive arthritis • The latent period between the antecedent streptococcal infection -migratory arthritis is shorter (1-2wks) than the 2-3 wks usually seen in ARF. • The response of arthritis to aspirin is poor • Evidence of carditis is not seen, and the severity of the arthritis is quite marked. • Extraarticular manifestations ie tenosynovitis & renal abnormalities often are seen . • Acute phase reactants (ESR, CRP) tend to be lower than of ARF.
- 19. End of slides Ref: • 1st slide pic :www.pathguy.com/lectures/heart.htm • Harrison’s Principles of Internal medicine • Davidson 21st ed • Uptodate 20.3 • Medscape
Editor's Notes
- Case scenario: a 15 yr old girl presented in opd by her mother with c/o involuntary movements of left hand.
- Acute rheumatic fever is a multisystem disorder that usually presents with fever, anorexia, lethargy and joint pain, 2-3 weeks after an episode of streptococcal pharyngitis. There may, however, be no history of sore throat. The diagnosis of ARF is established largely on clinical grounds. The initial description of clinical manifestations, known as the Jones criteria, were first published by Jones in 1944 and revised in 1965 . Subsequently, the American Heart Association (AHA) established guidelines for the diagnosis of rheumatic fever in 1992, and the Jones Criteria Working Group of the AHA reviewed this document in 2002 A presumptive diagnosis of acute rheumatic fever can be made without evidence of preceding streptococcal infection in cases of isolated chorea or pancarditis, if other causes for these have been excluded. In cases of established rheumatic heart disease or prior rheumatic fever, a diagnosis of acute rheumatic fever can be made based only on the presence of multiple minor criteria and evidence of preceding group A streptococcal pharyngitis. Fever is defined most often in ARF as typically body temperature of at least 39°C (≥102F) and occurring early in the course of disease. Arthralgia is defined as pain in one or more joints in the absence of polyarthritis as major criteria. Significantly if arthritis is noted as a major manifestation of the Jones criteria, arthralgia is not counted as a minor manifestation. Both acute-phase reactants, serum C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR) are raised in ARF (Serum CRP level of ≥30 mg/L or ESR of ≥ 30 mm/h). Both are invariably elevated during the active rheumatic phase unless they are suppressed by antirheumatic drug (Saxena et al., 2008). Among both the CRP is more useful because it typically normalize as soon as acute inflammation subsides but the ESR may stay elevated longer than 6 - 8 weeks after a transient inflammatory stimulus.
- Throat cultures are negative in about 75 percent . Anti-streptolysin O (ASO) titers vary with age, season, and geography . Healthy children of elementary school age commonly have titers of 200 to 300 Todd units per mL; Following streptococcal pharyngitis, the antibody response peaks at about four to five weeks, which usually is during the second or third week of rheumatic fever. Antibody titers fall off rapidly in the next several months and after six months have a slower decline. For these reasons, it may be useful to collect one specimen when the diagnosis of ARF is first suspected and another two weeks later. About 80 percent of patients with documented ARF demonstrate a rise in antistreptolysin titer, although this cannot be used as a measure of rheumatic activity. A negative antistreptolysin titer should prompt testing for other antistreptococcal antibodies such as anti-DNAse B (detectable for six to nine months following infection), streptokinase, and antihyaluronidase; Acute-phase reactants are increased in ARF. Both serum C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR) are invariably elevated during the active rheumatic process unless they are suppressed by antirheumatic drugs . CRP or ESR is useful for monitoring "rebounds" of inflammation as treatment is tapered. A normal result obtained a few weeks after discontinuing antirheumatic therapy suggests that the course of the illness is complete (unless chorea appears). The CRP is probably more useful since it typically normalizes over a matter of days once an episode of acute inflammation has resolved, while the ESR may stay elevated for up to two months after a transient inflammatory stimulus. A mild normochromic normocytic anemia of chronic inflammation may be observed during acute rheumatic fever. Suppressing the inflammation usually improves the anemia; Complement levels are usually normal in ARF. In contrast, hypocomplementemia is typically observed in the setting of poststreptococcal glomerulonephritis. Analysis of the synovial fluid in rheumatic fever with arthritis generally demonstrates sterile inflammatory fluid.
- In the absence of pericarditis or involvement of a new valve, it may be difficult establish a diagnosis of acute carditis during an acute attack. Therefore, a presumptive diagnosis of recurrent acute rheumatic fever may be made with one major or two minor criteria if there is evidence of a recent group A streptococcal infection. Caution against using a single clinical finding (eg, monoarthritis, fever, arthralgia) as a criterion for the diagnosis of recurrent disease has been suggested
- Its incidence declines with increasing age, ranging from 90% at 3 years to around 30% in adolescence. ECG changes commonly include ST and T wave changes. Conduction defects sometimes occur and may cause syncope.
- The natural history of arthritis due to RF consists of inflammation affecting several joints in quick succession, each lasting for a few days to a week . The knees, ankles, elbows, and wrists are affected most commonly; the leg joints are typically involved first. The onset of arthritis in different joints usually overlaps, giving the appearance that the disease "migrates" from joint to joint. Thus, the terms "migrating" or "migratory" are used to describe the polyarthritis of rheumatic fever. Onset and resolution of arthritis may be rapid (within 1 to 2 days) and the arthritis may be severe enough to severely limit movement. Arthritis usually is the earliest symptomatic manifestation of ARF, although asymptomatic carditis may develop first. Radiography of an affected joint may demonstrate a slight effusion but is usually unremarkable. Analysis of the synovial fluid in rheumatic fever with arthritis generally demonstrates sterile inflammatory fluid. Etc: Calor, dolor, rubor, and tumor: Heat, pain, redness, and swelling. The four classical signs of inflammation, originally recorded by the Roman encyclopedist Celsus in the 1st century A.D. Functio laesa is a term used in medicine to refer to a loss of function or a disturbance of function.It was identified as the fifth sign of acute inflammation by Galen.
- Erythema marginatum — Erythema marginatum is an evanescent, pink or faintly red, non-pruritic rash involving the trunk and sometimes the limbs but not the face . The lesion extends centrifugally with return of the skin in the center to a normal appearance. The outer edge of the lesion is sharp; the inner edge is diffuse. The lesion is also known as "erythema annulare" since the margin of the lesion is usually continuous, making a ring . Individual lesions may appear, disappear, and reappear in a matter of hours. A hot bath or shower may make them more evident. Erythema marginatum usually occurs early in the course of ARF in patients with acute carditis, but may persist or recur when all other manifestations of disease have disappeared . Cases have been reported in patients with chronic carditis . In some cases the lesions are first noticed late in the course of the illness or even during convalescence. Subcutaneous nodules — Subcutaneous nodules in ARF are firm, painless lesions ranging from a few millimeters to 2 cm in size. The nodules are usually located over a bony surface or prominence or near tendons (usually extensor surfaces) and are usually symmetric. The overlying skin is not inflamed and usually can be moved over the nodules . The number of nodules varies from a single lesion to a few dozen; the average number is three or four. Rheumatic subcutaneous nodules generally appear after the first weeks of illness, usually in patients with relatively severe carditis. Typically nodules are present for one or more weeks; they rarely persist for more than a month. Nodules of ARF are smaller and more short-lived than the nodules of rheumatoid arthritis. The elbows are involved most frequently in both rheumatic fever and rheumatoid arthritis; they may be distinguished in that rheumatic fever nodules occur most commonly on the olecranon, while rheumatoid nodules usually are found 3 to 4 cm distally. In contemporary outbreaks of ARF, nodules have been the least common manifestation (less than 5 percent of patients)
- sydenham chorea (also known as chorea minor or "St. Vitus dance") is a neurologic disorder consisting of abrupt, nonrhythmic involuntary movements, muscular weakness, and emotional disturbances . Neurologic examination fails to reveal sensory losses or involvement of the pyramidal tract. The movements frequently are more marked on one side, are occasionally unilateral (hemichorea), and cease during sleep. Muscle weakness is best demonstrated by asking the patient to squeeze the examiner's hands. The pressure of the patient's grip increases and decreases capriciously, a phenomenon known as relapsing grip or "milk maids sign." Diffuse hypotonia may be present. Emotional changes manifest with outbursts of inappropriate behavior including crying and restlessness. In rare cases, psychologic manifestations are severe and may result in transient psychosis. Chorea can present up to eight months after streptococcal infections; this is a longer latent period than other rheumatic manifestations . Some patients with chorea have no other clinical symptoms but should undergo evaluation for carditis with echocardiogram.
- A single dose of benzyl penicillin 1.2 million U i.m. or oral phenoxymethylpenicillin 500 mg 12-hourly for 10 days should be given on diagnosis to eliminate any residual streptococcal infection. If the patient is penicillin-allergic, erythromycin or a cephalosporin can be used. Treatment is then directed towards limiting cardiac damage and relieving symptoms. Bed rest and supportive therapy Bed rest is important, as it lessens joint pain and reduces cardiac workload. The duration should be guided by symptoms along with temperature, leucocyte count and ESR, and should be continued until these have settled. Patients can then return to normal physical activity but strenuous exercise should be avoided in those who have had carditis. Cardiac failure should be treated as necessary. Some patients, particularly those in early adolescence, develop a fulminant form of the disease with severe mitral regurgitation and sometimes concomitant aortic regurgitation. If heart failure in these cases does not respond to medical treatment, valve replacement may be necessary and is often associated with a dramatic decline in rheumatic activity. AV block is seldom progressive and pacemaker insertion rarely needed. Aspirin This will usually relieve the symptoms of arthritis rapidly and a response within 24 hours helps to confirm the diagnosis. 4-8 gm /d in 5 divided dosage.Mild toxic effects include nausea, tinnitus and deafness; vomiting, tachypnoea and acidosis are more serious. Aspirin should be continued until the ESR has fallen and then gradually tailed off. Corticosteroids These produce more rapid symptomatic relief than aspirin and are indicated in cases with carditis or severe arthritis. There is no evidence that long-term steroids are beneficial. Prednisolone, 1.0-2.0 mg/kg per day in divided doses, should be continued until the ESR is normal then tailed off
- Patients are susceptible to further attacks of rheumatic fever if another streptococcal infection occurs, and long-term prophylaxis with penicillin should be given as benzathine penicillin 1.2 million U i.m. monthly (if compliance is in doubt) or oral phenoxymethylpenicillin 250 mg 12-hourly. Sulfadiazine or erythromycin may be used if the patient is allergic to penicillin; sulphonamides prevent infection but are not effective in the eradication of group A streptococci. Further attacks of rheumatic fever are unusual after the age of 21, when treatment may be stopped. However, it should be extended if an attack has occurred in the last 5 years, or if the patient lives in an area of high prevalence or has an occupation (e.g. teaching) with high exposure to streptococcal infection. In those with residual heart disease, prophylaxis should continue until 10 years after the last episode or 40 years of age, whichever is longer. Long-term antibiotic prophylaxis prevents another attack of acute rheumatic fever but does not protect against infective endocarditis.
- Rheumatic heart disease is the most severe sequela of acute rheumatic fever. It usually occurs 10 to 20 years after the original illness and is the most common cause of acquired valvular disease in the world . The main pathological process in chronic rheumatic heart disease is progressive fibrosis. The heart valves are predominantly affected but involvement of the pericardium and myocardium may contribute to heart failure and conduction disorders. Fusion of the mitral valve commissures and shortening of the chordae tendineae may lead to mitral stenosis with or without regurgitation. Similar changes in the aortic and tricuspid valves produce distortion and rigidity of the cusps, leading to stenosis and regurgitation. Once a valve has been damaged, the altered haemodynamic stresses perpetuate and extend the damage, even in the absence of a continuing rheumatic process.
- Several investigators have speculated that some cases of arthritis occurring after a streptococcal infection may not be caused by ARF. This disorder has been called poststreptococcal reactive arthritis (PSRA) )