Downloaded 12 times

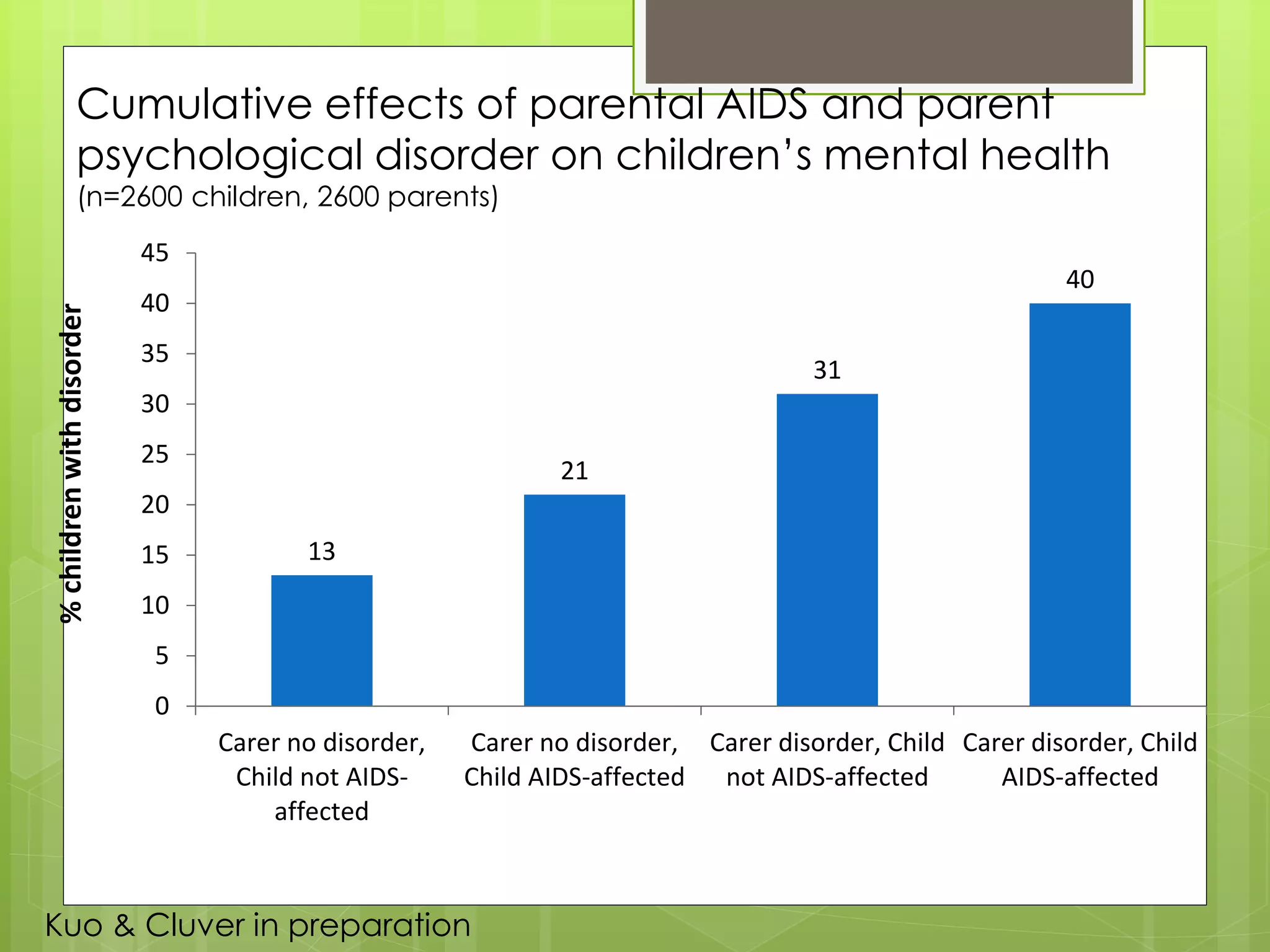
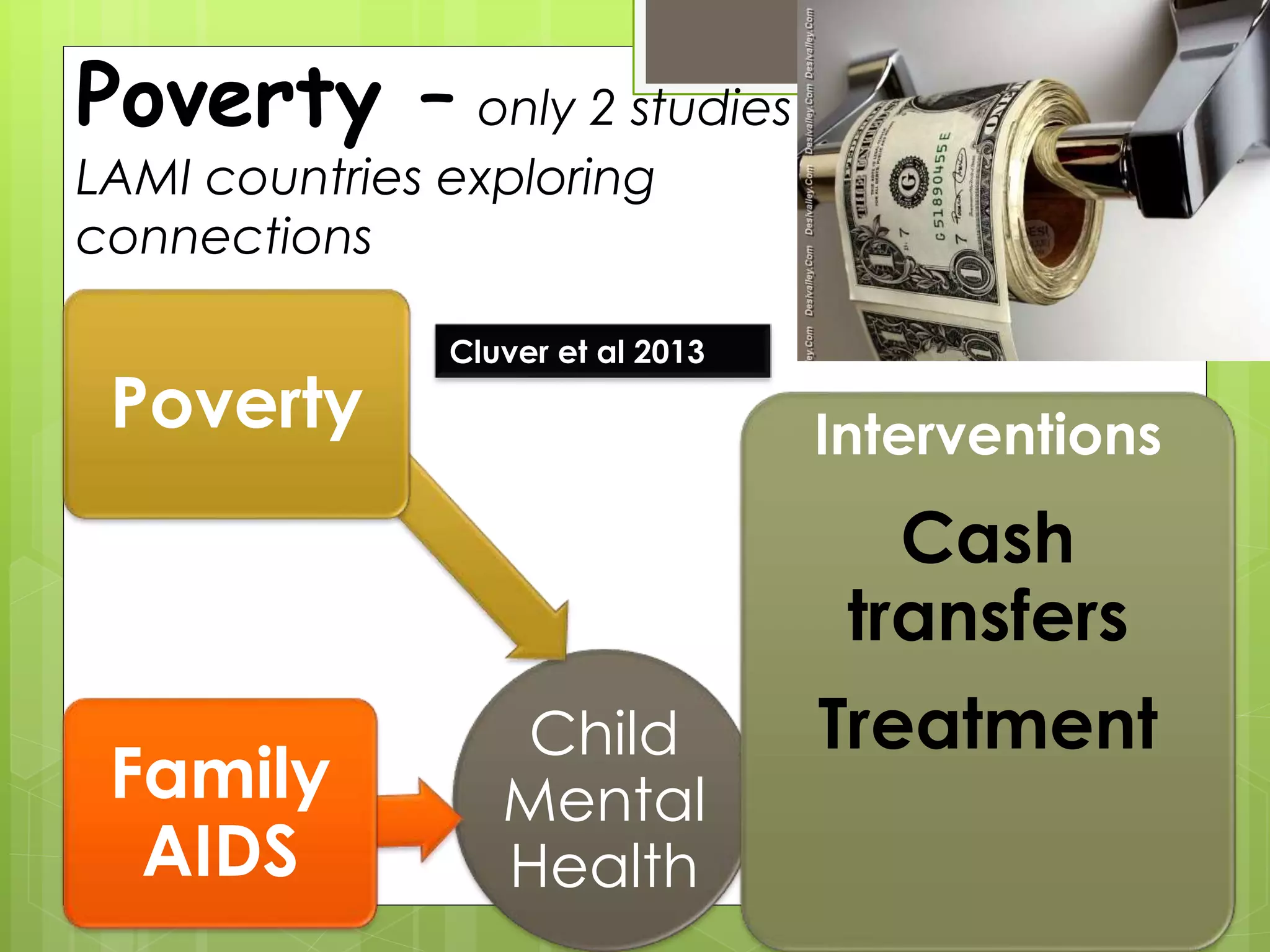
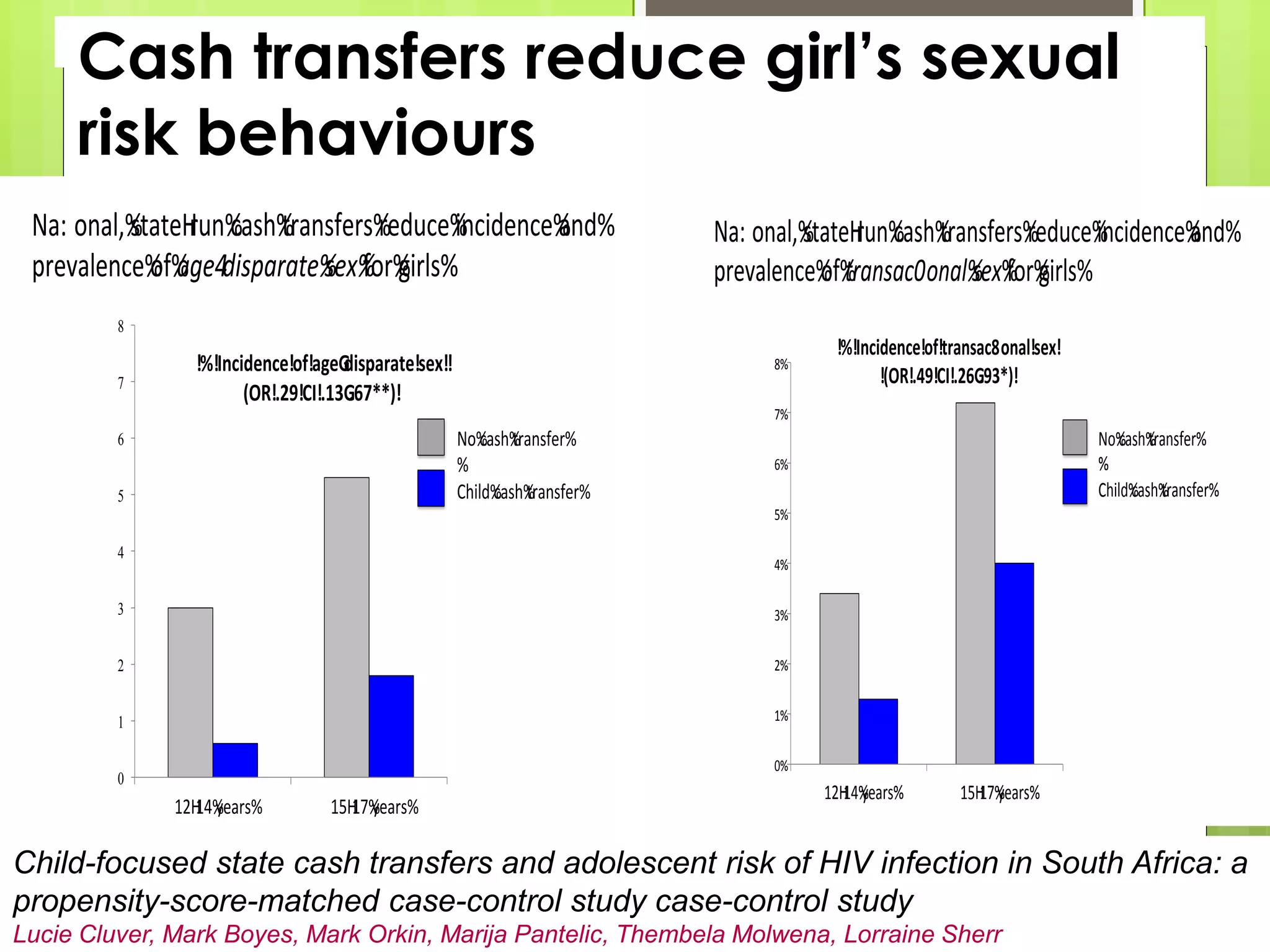
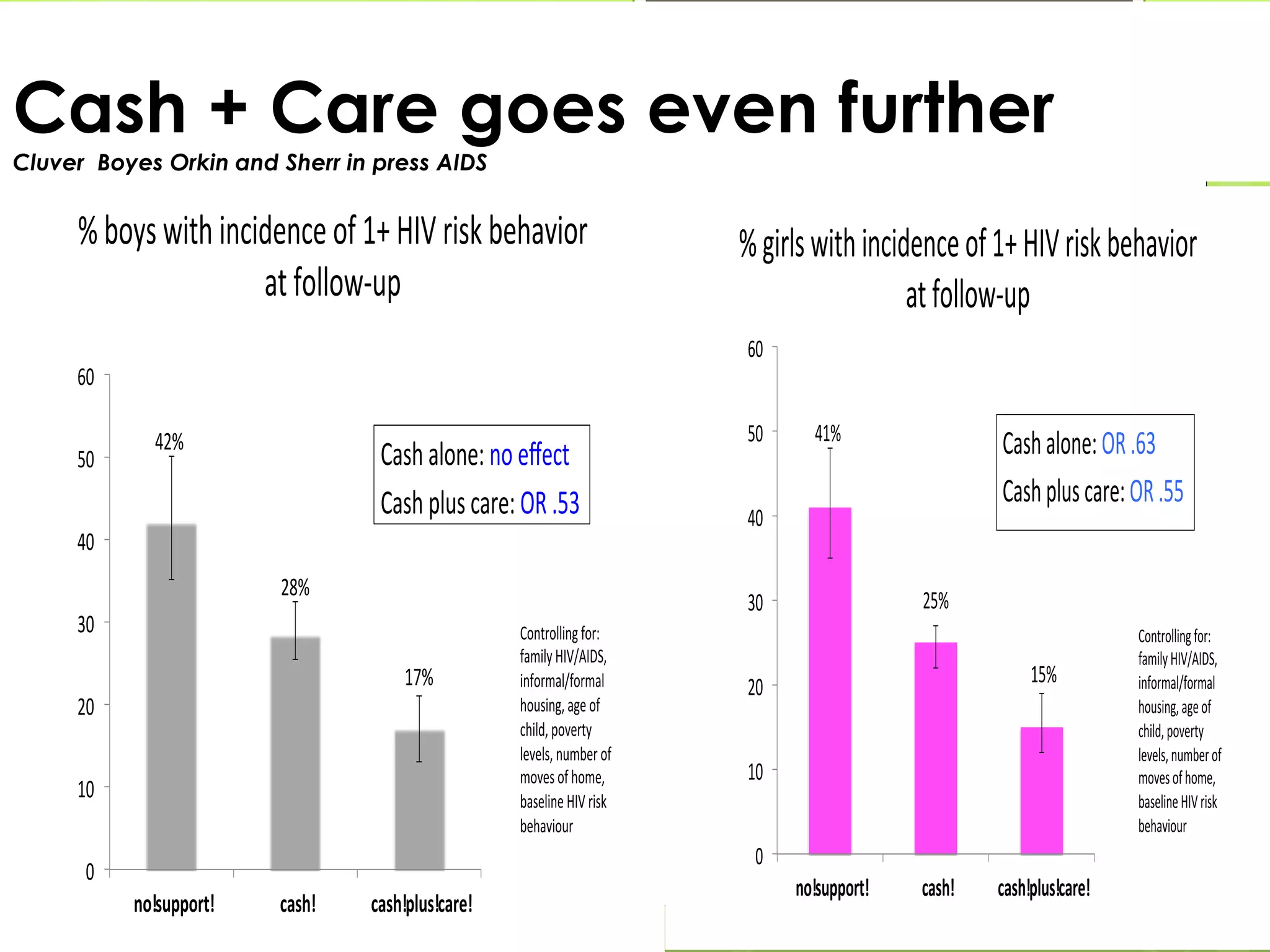

The document discusses the critical role of parenting in the context of HIV, emphasizing the need for parental support to prevent vertical transmission and enhance child well-being. It highlights the significant mental and physical health challenges faced by parents living with HIV, which in turn affect their children. Furthermore, it stresses the importance of stable family structures and interventions such as cash transfers to improve outcomes for children affected by HIV.





















































![Exploring the cinderella_myth__intrahousehold.11[1]](https://cdn.slidesharecdn.com/ss_thumbnails/exploringthecinderellamythintrahousehold-111-100908035327-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















