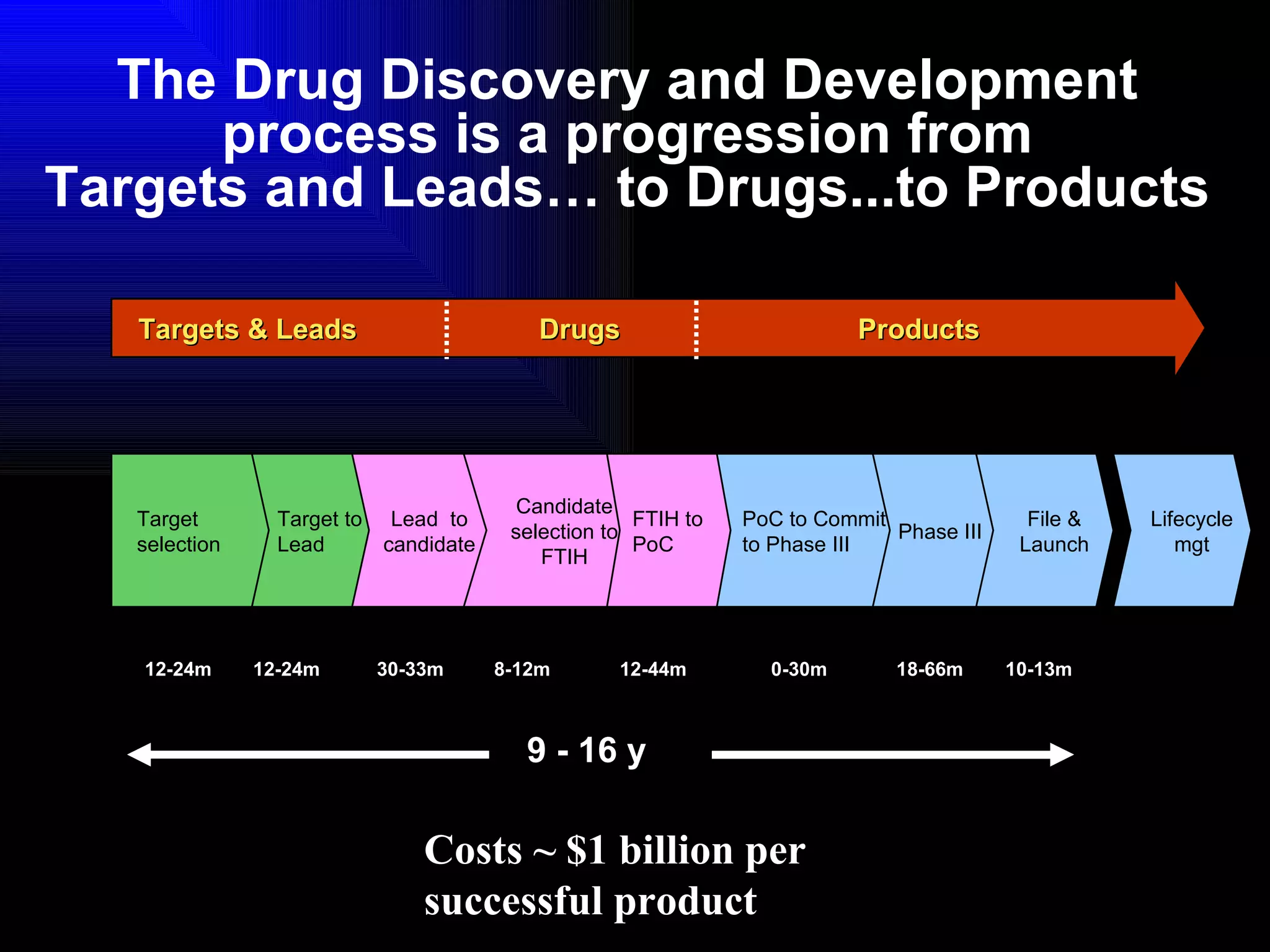
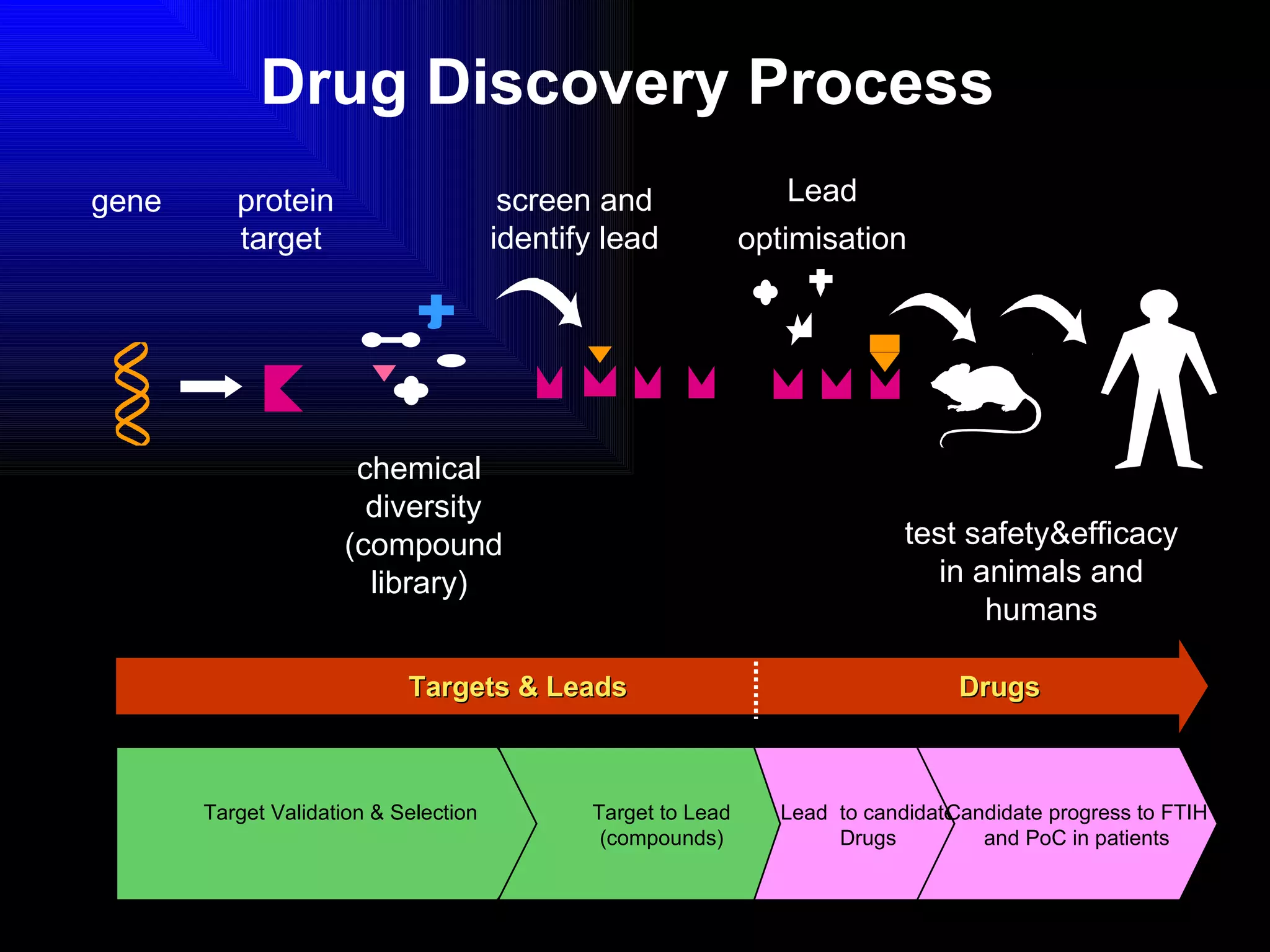
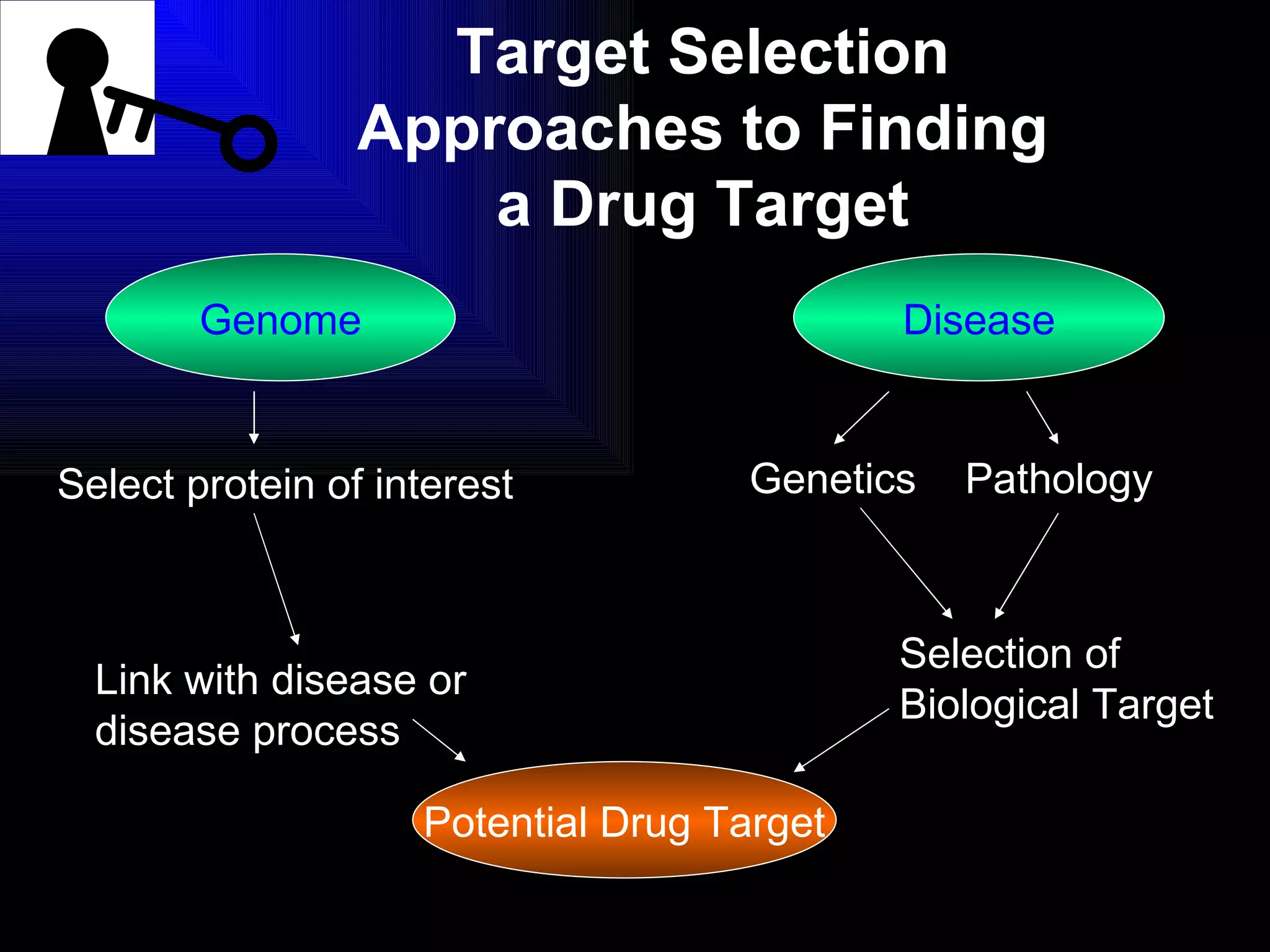
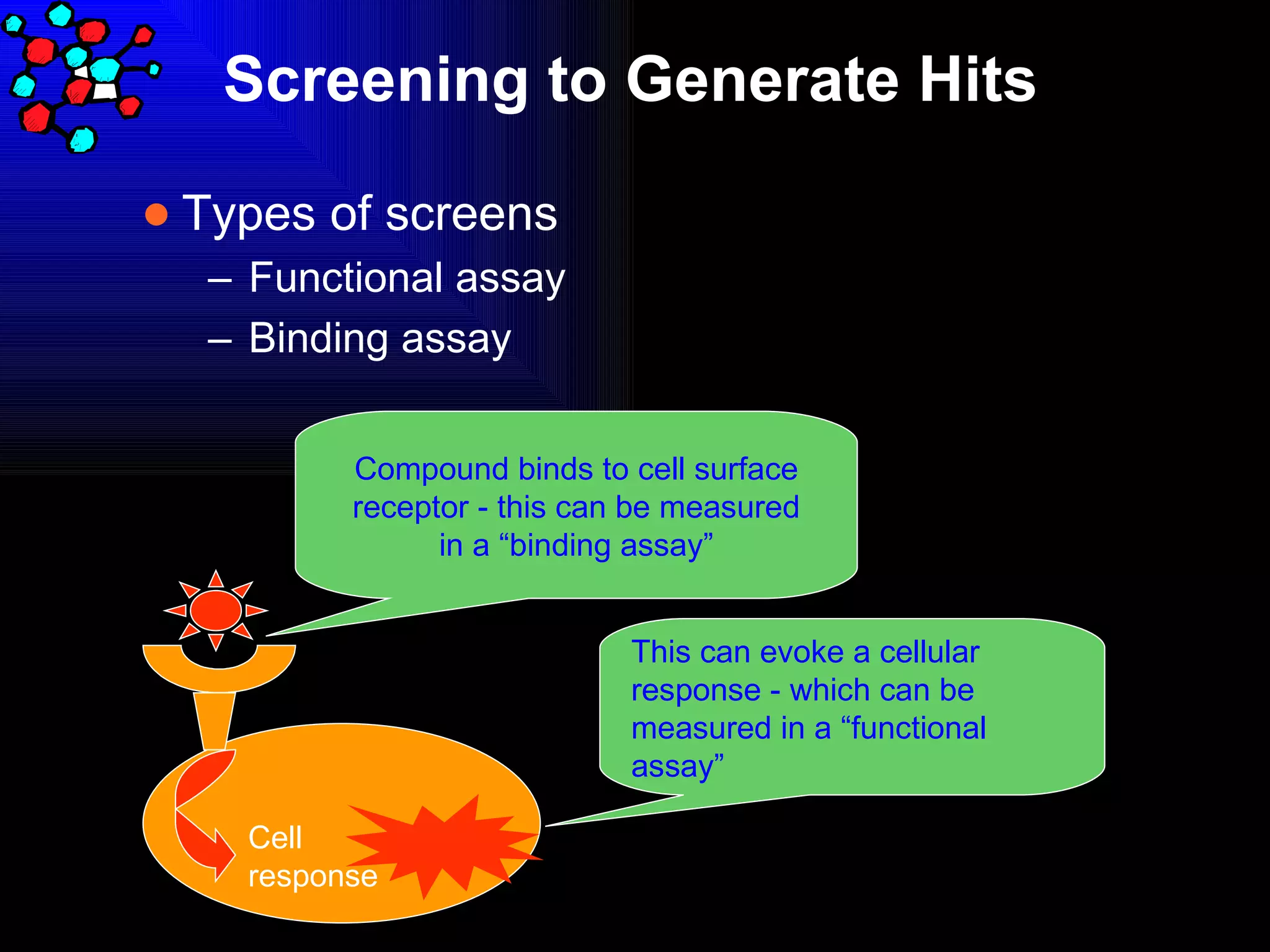
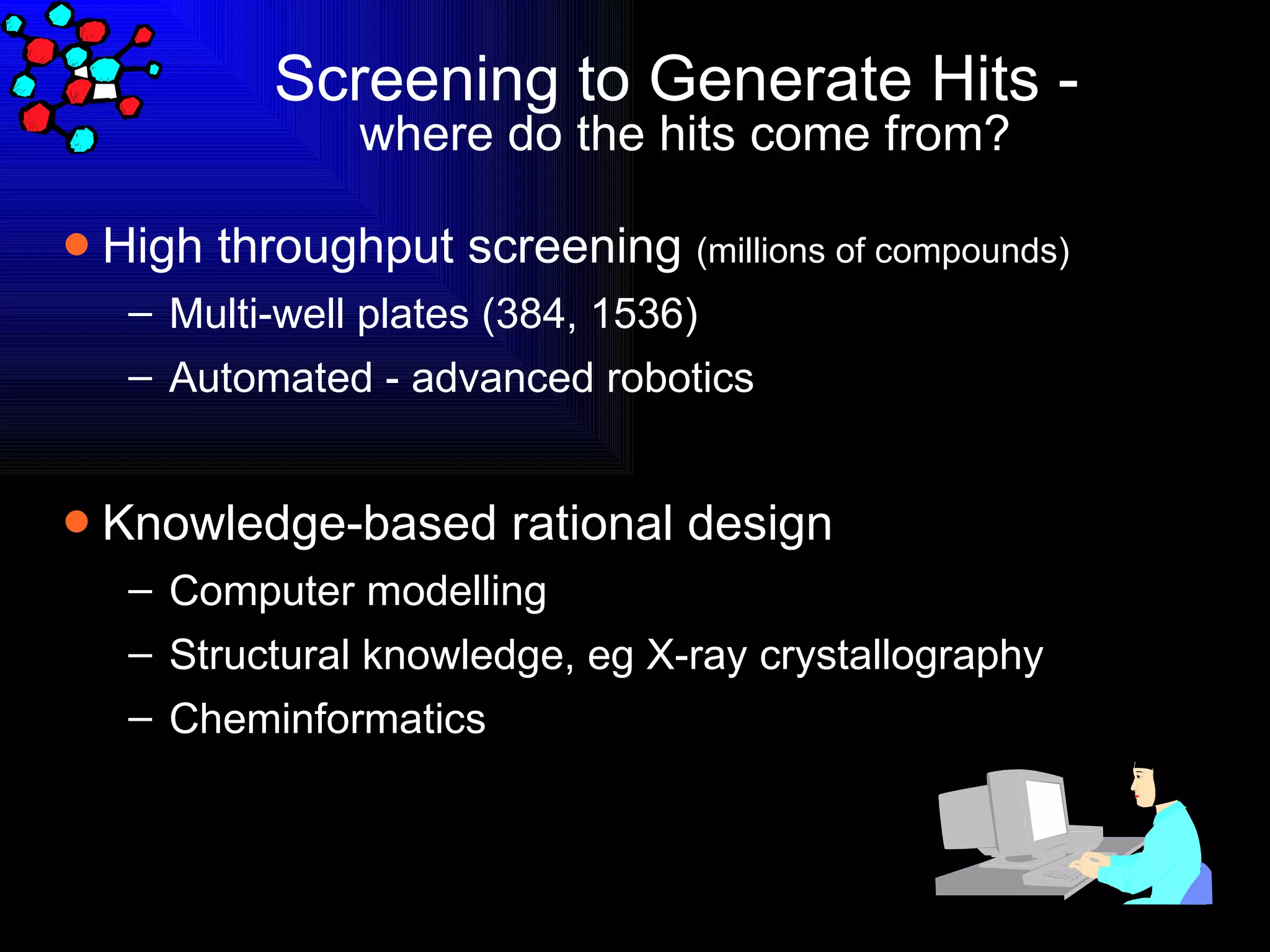
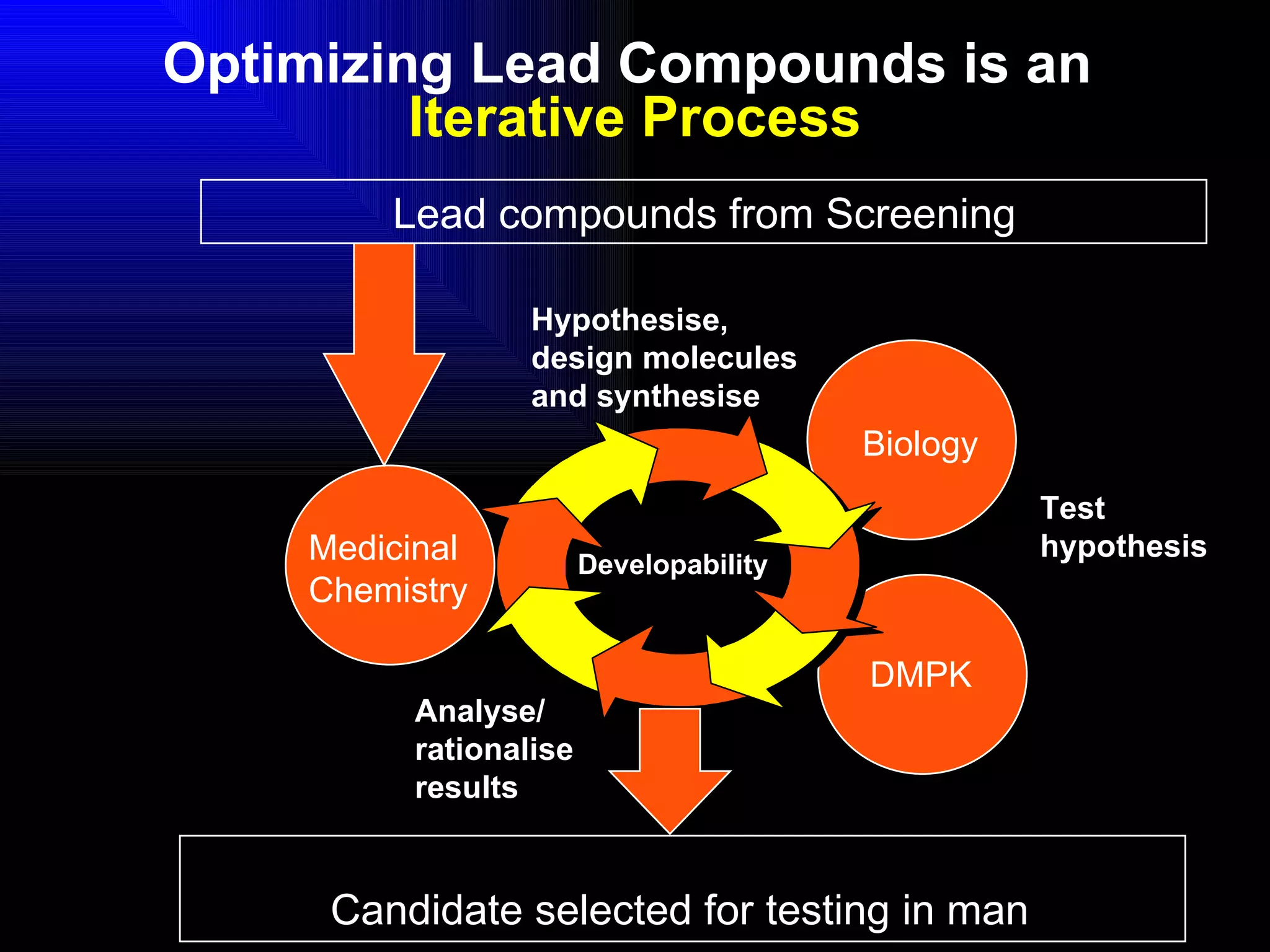
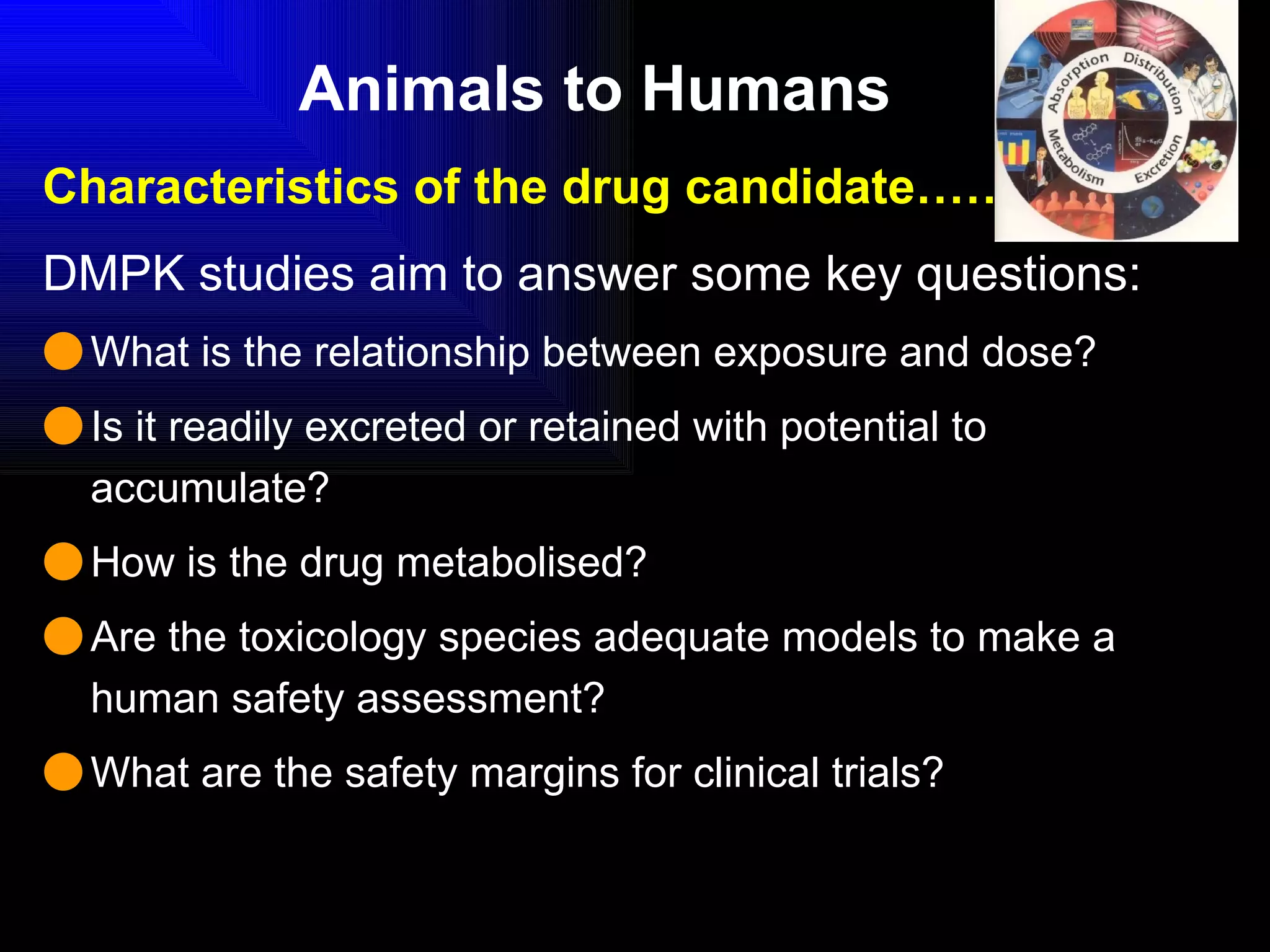
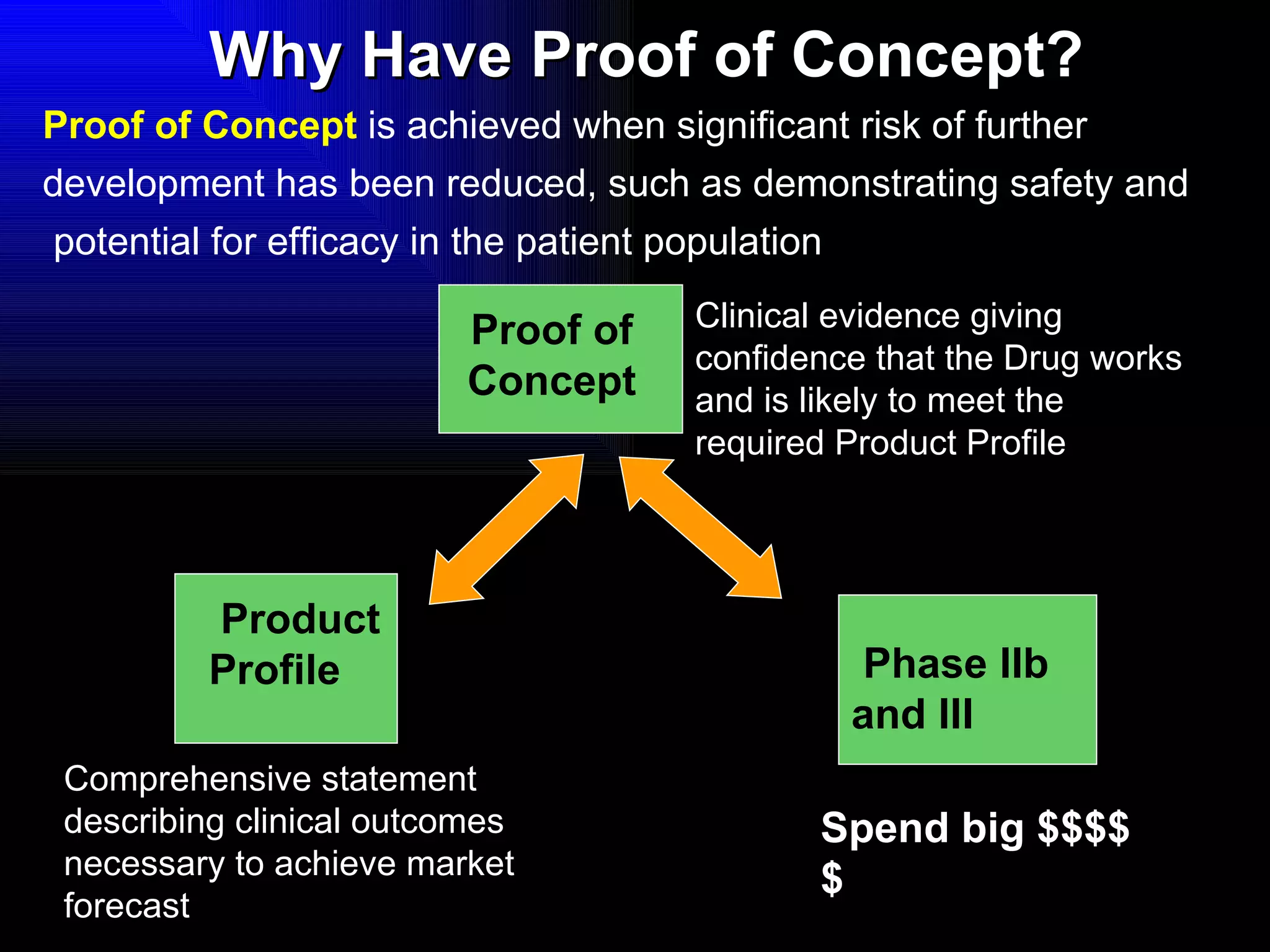
The document discusses the key stages in the drug discovery and development process including target selection, compound screening and hit optimization, selecting a drug candidate through further optimization of properties like absorption and metabolism, safety testing in animals and humans, proof of concept clinical trials in patients, large phase 3 clinical trials for registration and approval, and finally launch and life cycle management. It notes that the entire process from discovery to approval can take 12-16 years and cost over $1 billion.




















![Abbreviated New Drug Application [ANDA]](https://cdn.slidesharecdn.com/ss_thumbnails/abbreviatednewdrugapplicationanda-160619062810-thumbnail.jpg?width=640&height=640&fit=bounds)
















![Preclinical_Phase_of_Drug_Development_Lucas[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/preclinicalphaseofdrugdevelopmentlucas1-251107071109-7c5cab19-thumbnail.jpg?width=640&height=640&fit=bounds)









