Madura foot ppt

Definition: Madura foot or mycetoma (tumour-like) Chronic granulomatous disease characterised by localised infection of subcutaneous tissues and sometimes bone characterised by discharging sinuses filled with organisms like actinomycetes or fungi. History: Gill first described the disease in the Madura district of India in 1842. Hence the term Madura foot. Pathophysiology:Typically present in agricultural workers(hands shoulders and back – from carrying contaminated vegetation and other burdens). Causes:Due to fungi – eumycetoma (40%) or Actinomycetes – (actinomycetoma) 60% Actinomycetoma may be due to Actinomadura madurae Actinomadura pelletieri Streptomyces somaliensis Nocardia species Clinical Features:Slow spreading skin infection Local swelling Small hard painless nodules Ulceration Pus discharge Scarred skin & discoloration Itching Pain and burning sensation Lab studies:Direct microscopy Blood – leukocytosis & neutrophilia Culture of exudates Skin biopsy Serology DNA sequencing has been used for identification in difficult cases. Microscopy:Serosanguinous fluid containing the granules examined using – 10% KOH and Parker ink or calcofluor white mounts Tissue sections stained using H&E(Hematoxylin and Eosin stain) , PAS(Periodic Acid Shiffs Stain) and Grocott’s methenamine silver(GMS). Actinomycotic grains contains very fine filaments. Fungal grains contain short hyphae (branched filaments) that are often swollen Culture:Sabouraud’s dextrose agar or mycobiotic agar to isolate fungi Blood agar to isolate bacteria Agar plates are cultured at 25-30 degree celcius and 37 degree celcius for up to six weeks . Fungi grow more quickly than actinomycetes. Treatment;Due to the slow ,relatively pain –free progression of the disease, mycetoma is often at an advanced stage when diagnosed. Antifungals Antibiotics Treatment of any secondary infections Amputation-in severe cases

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Madura foot ppt
Similar to Madura foot ppt (20)
More from thirupathiSathya
More from thirupathiSathya (18)
Recently uploaded
Recently uploaded (20)
Madura foot ppt
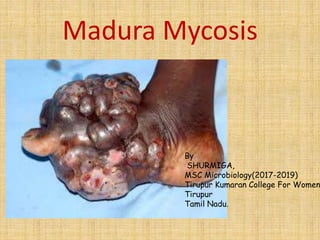
- 1. Madura Mycosis By SHURMIGA, MSC Microbiology(2017-2019) Tirupur Kumaran College For Women Tirupur Tamil Nadu.
- 2. Definition • Madura foot or mycetoma (tumour-like) • Chronic granulomatous disease characterised by localised infection of subcutaneous tissues and sometimes bone characterised by discharging sinuses filled with organisms like actinomycetes or fungi.
- 3. History • Gill first described the disease in the Madura district of India in 1842. • Hence the term Madura foot.
- 4. Pathophysiology • Typically present in agricultural workers(hands shoulders and back – from carrying contaminated vegetation and other burdens).
- 5. • Individuals who walk barefoot in dry , dusty conditions • People who work in rural areas where they are exposed to acacia trees or cactus thorns containing the etiologic agents.
- 6. • Spread occurs through skin facial planes and can involve the bone. • Two thirds arise on the foot , but can involve the hands , back or shoulders. • Following initial injury , the disease – follows a slow chronic course over many years with painless swelling and intermittent discharge of pus.
- 7. • There may be a deep itching sensation • Pain may occur due to secondary bacterial infection or bone invasion • After some years, massive swelling of the area occurs , with induration , skin rupture and sinus trace formation. As the infection spreads, old sinuses close and new ones open
- 10. Causes • Due to fungi – eumycetoma (40%) or • Actinomycetes – (actinomycetoma) 60% • Actinomycetoma may be due to Actinomadura madurae Actinomadura pelletieri Streptomyces somaliensis Nocardia species
- 11. • Eumycetoma is often due to Madurella mycetomi , Pseudallescheria boydi (Scedosporium apiospermum) , Cladophialophora
- 14. Clinical features • Slow spreading skin infection • Local swelling • Small hard painless nodules • Ulceration • Pus discharge • Scarred skin & discoloration • Itching • Pain and burning sensation
- 17. Lab studies • Direct microscopy • Blood – leukocytosis & neutrophilia • Culture of exudates • Skin biopsy • Serology • DNA sequencing has been used for identification in difficult cases.
- 18. Microscopy • Serosanguinous fluid containing the granules examined using – 10% KOH and Parker ink or calcofluor white mounts • Tissue sections stained using H&E(Hematoxylin and Eosin stain) , PAS(Periodic Acid Shiffs Stain) and Grocott’s methenamine silver(GMS). • Actinomycotic grains contains very fine filaments. • Fungal grains contain short hyphae (branched filaments) that are often swollen
- 22. Culture • Sabouraud’s dextrose agar or mycobiotic agar to isolate fungi • Blood agar to isolate bacteria • Agar plates are cultured at 25-30 degree celcius and 37 degree celcius for up to six weeks . Fungi grow more quickly than actinomycetes.
- 24. Serology • (1) Immunodiffusion tests eumycotic mycetoma infections. • (2) Counterimmunoelectrophoresis • (3) Enzyme-linked immunosorbent assay (ELISA) • (4) Western blot.
- 25. Imaging • Plain x-rays assess for evidence of bone involvement • CT scan may be more sensitive in the early stages • MRI scans better assessment of the degree of bone and soft tissue involvement; and may be useful in evaluating the differential diagnosis of the swelling .
- 26. Bone radiography • Once mycetoma has invaded the bone, the following changes may be observed: • Cortical thinning is due to compression from the outside by the mycetoma. • Multiple lytic lesions or cavities may be large and few in number with well-defined margins (eumycetoma) or small and numerous with ill defined margins(actinomycetoma). • Osteoporosis may occur in late stages.
- 28. Ultrasonography • Single or multiple thick-walled cavities with hyper reflective echoes and no acoustic enhancement • In eumycetoma, the hyper reflective echoes are sharp, corresponding to the grains in the lesion. • In actinomycetoma, the hyper effective echoes are fine and closely aggregated and commonly settle at the bottom of the cavities.
- 30. Treatment Due to the slow ,relatively pain –free progression of the disease, mycetoma is often at an advanced stage when diagnosed. • Antifungals • Antibiotics • Treatment of any secondary infections • Amputation-in severe cases
- 31. Amputation
- 32. Medical • Actinomycetomas usually respond better to medical treatment than eumycetomas • Therapy is suggested for 1-2 years (or greater) for complete eradication • The current treatment of actinomycetoma is trimethoprim-sulfamethoxazole 7.5-40mg/kg daily in 3 oral doses for several months or years.
- 33. Eumycetoma • Ketoconazole 400mg daily • Itraconazole 300mg daily • Amphotericin B 50 mg daily • Terbinafine • External beam radiotherapy in doses ranging from 3.5-14 Gy has been considered successful treatment in a few selected cases.
- 35. Surgical • Excision of the affected tissues • Localized mycetoma lesions that can be excised completely without residual disability. • Disease process more extensive than suggested by superficial lesion- so apparently healthy tissue removed to avoid recurrence • Surgical reduction of large lesions can improve the patient’s response to medical treatment.
- 36. • Scalp lesion- rapidly fatal so attended without delay • Extensive surgery may have to be followed by skin grafting/plastic surgery • To cover large open area /improve functions • Extensive bone involvement often warrents surgical amputation.
- 37. Complications • Secondary bacterial infection • Immonucompromised patients may can develop invasive infection • This can cause increased pain and disability as well as osteomyelitis, septicaemia, which my be fatal if untreated. • Lymphatic obstruction and fibrosis may cause lymph oedema • In advanced cases, deformities or ankylosis may occur • Chronic neglected infection may necessitate amputation.
- 38. • Complications may result from toxicity due to prolonged antimicrobial of antifungal therapy. • Actinomycetoma can be cured with the appropriate antibiotic therapy but eumycetoma has a high rate of recurrence and can require amputation.
- 39. Epidemology • Endemic in the tropics and subtropics • More common in men than in women • The male-to-female ratio is 3:1 • Particularly those aged 20 to 50
- 40. Madura foot