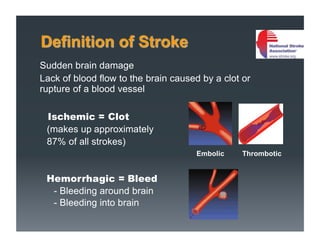
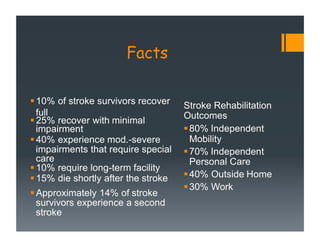
1) Stroke is caused by lack of blood flow to the brain due to a clot or ruptured blood vessel. It can cause disabilities like paralysis, sensory issues, language problems, and cognitive impairments.
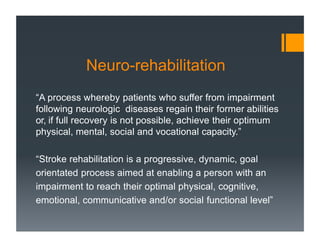
2) Stroke rehabilitation aims to help survivors regain abilities or achieve their optimal functioning through a goal-oriented process. This is done by leveraging neuroplasticity, where the brain can change and adapt in response to cues.
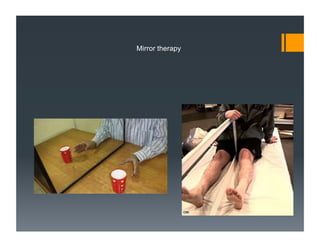
3) Newer developments in stroke rehabilitation techniques leverage the principles of neuroplasticity, such as constraint-induced movement therapy, mirror therapy, and sensory stimulation to enhance recovery.











































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)