Downloaded 61 times



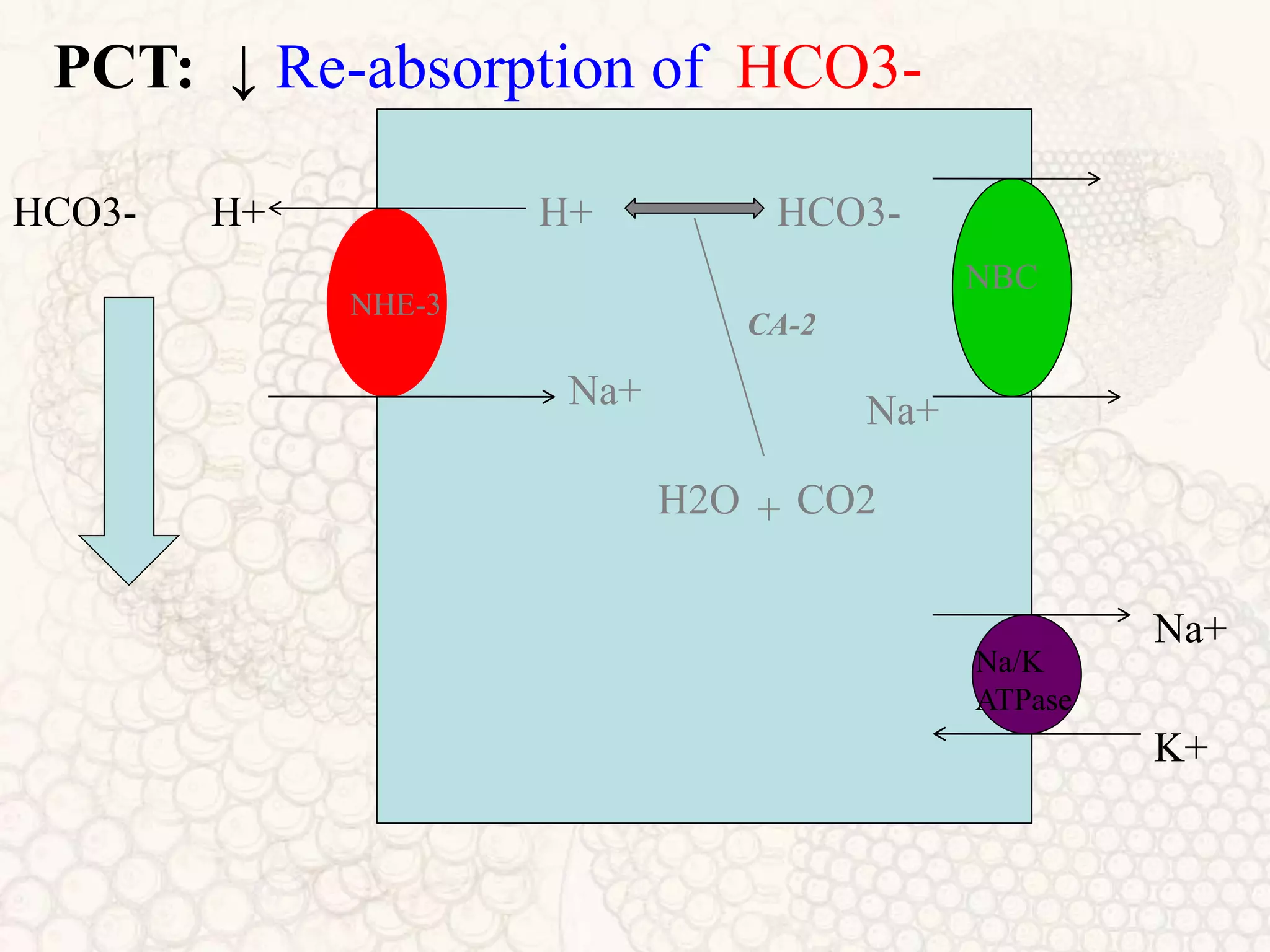


















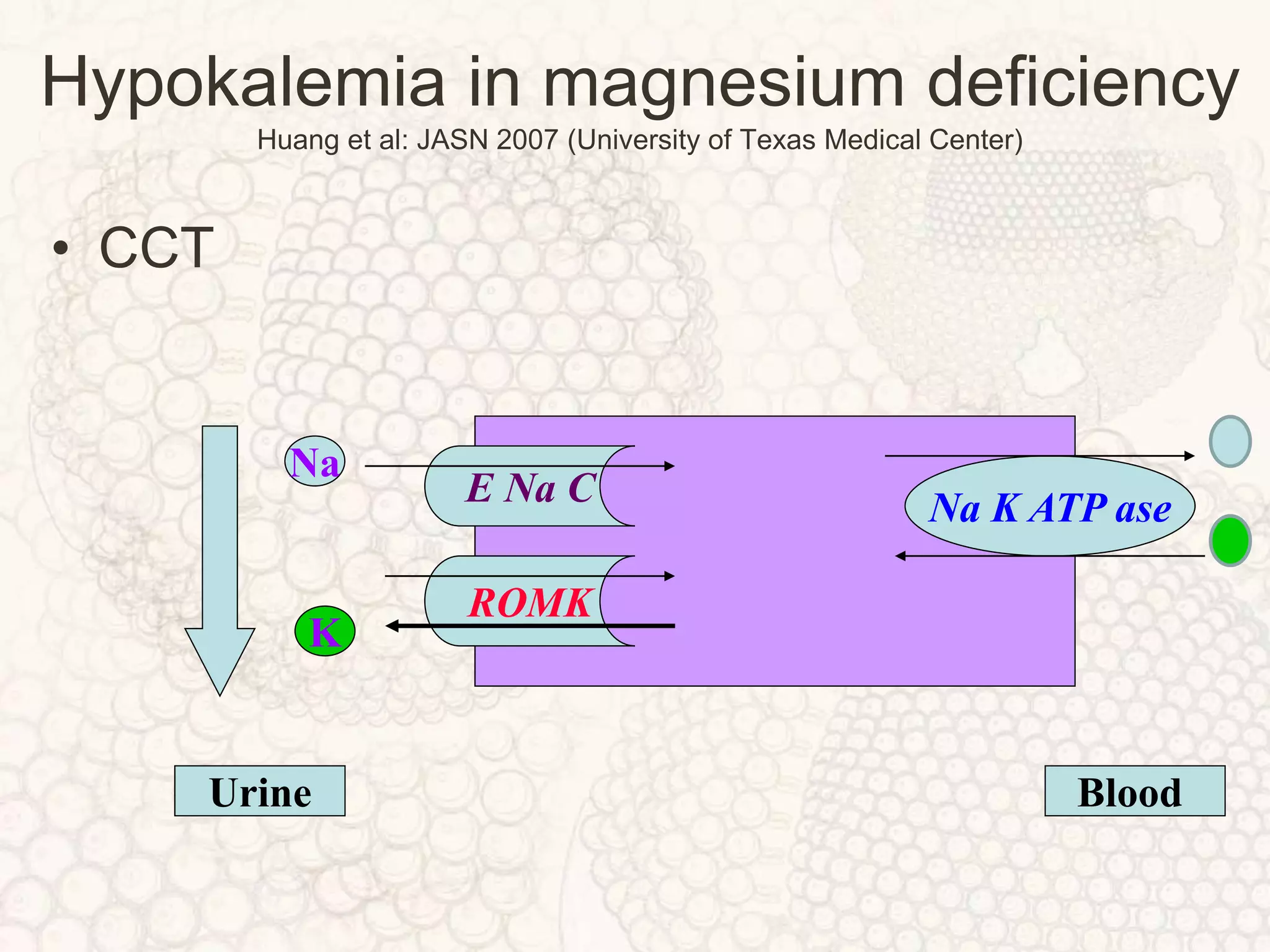
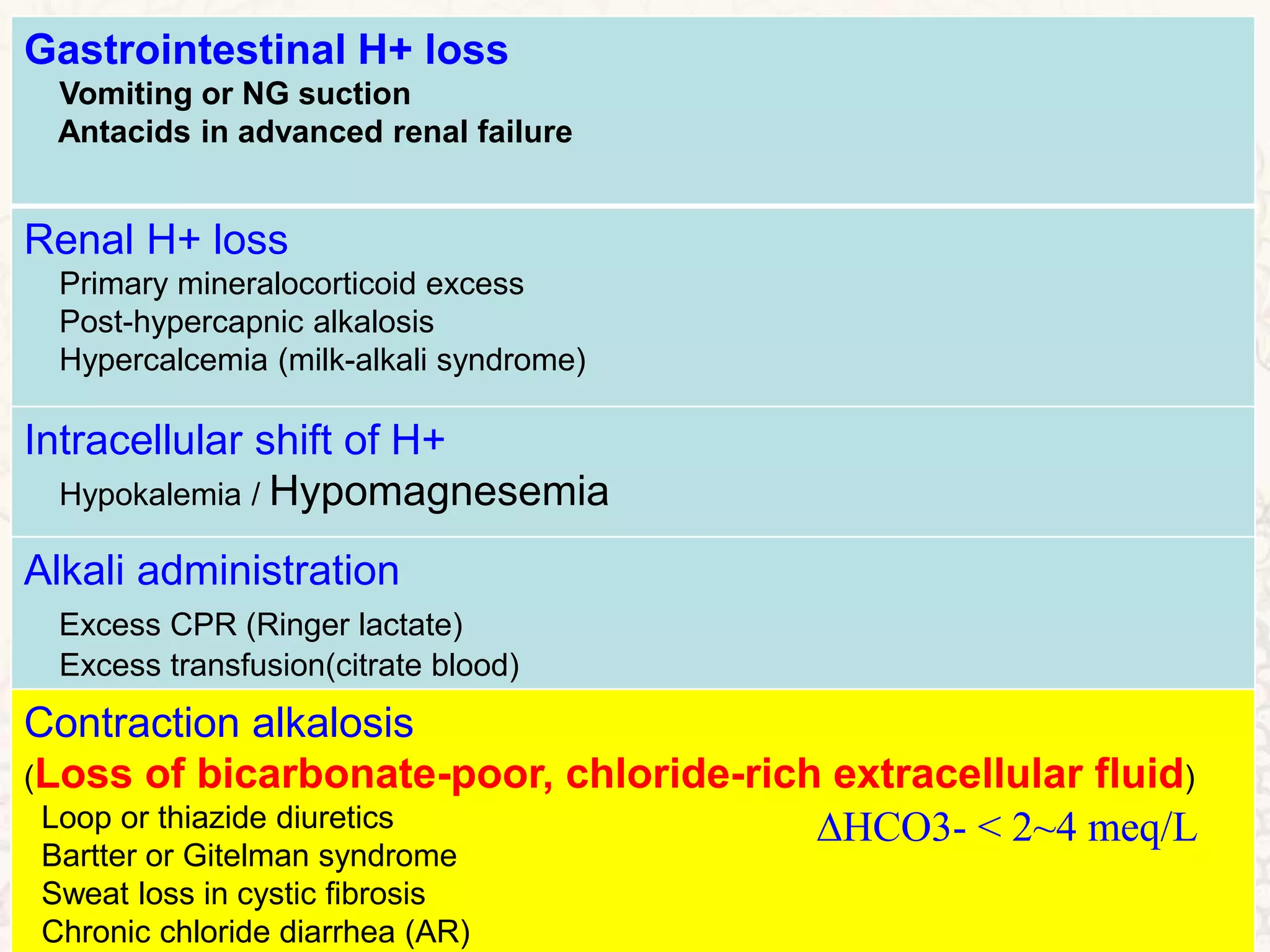




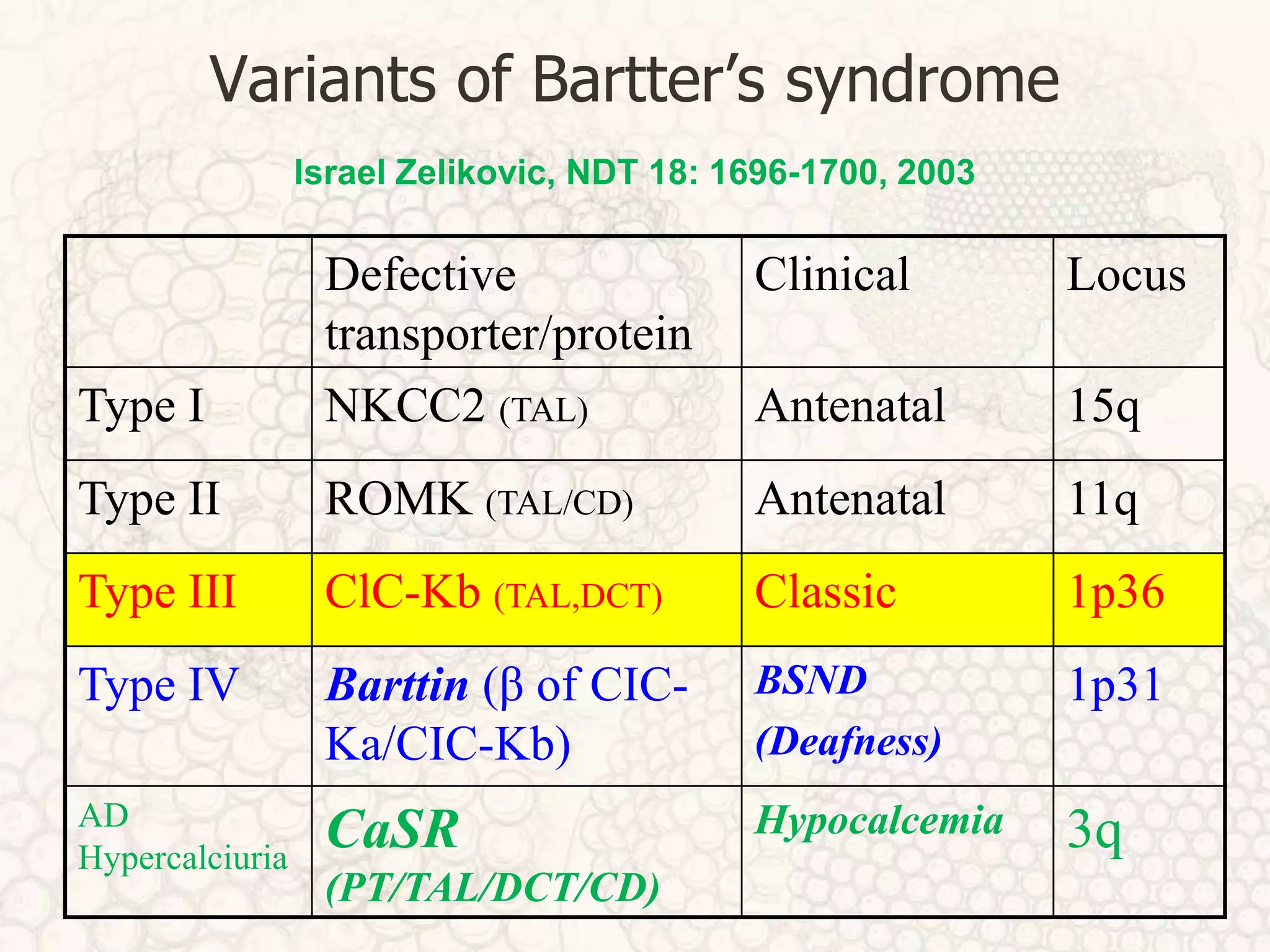




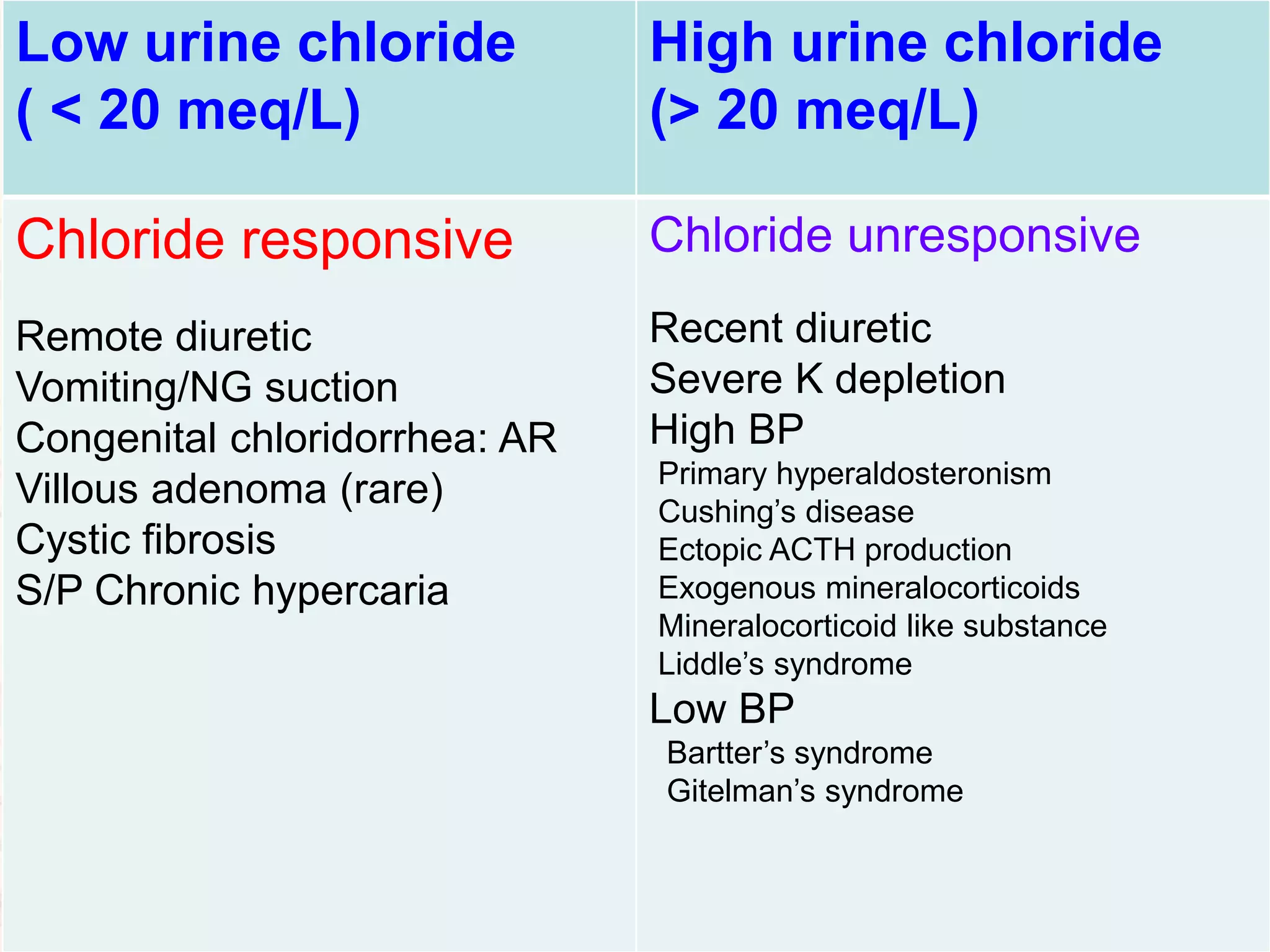













The document discusses metabolic alkalosis, outlining the mechanisms that can cause increased bicarbonate levels including hypokalemia, hypomagnesemia, corticosteroid excess, and gastrointestinal or renal losses of hydrogen ions. It examines these mechanisms in detail through their effects on ion transporters in the kidney, and explores related conditions like Bartter syndrome, Gitelman syndrome, and mineralocorticoid excess. General principles for treatment focus on increasing renal bicarbonate excretion and addressing underlying causes of potassium depletion or reduced effective arterial blood volume.