Downloaded 30 times

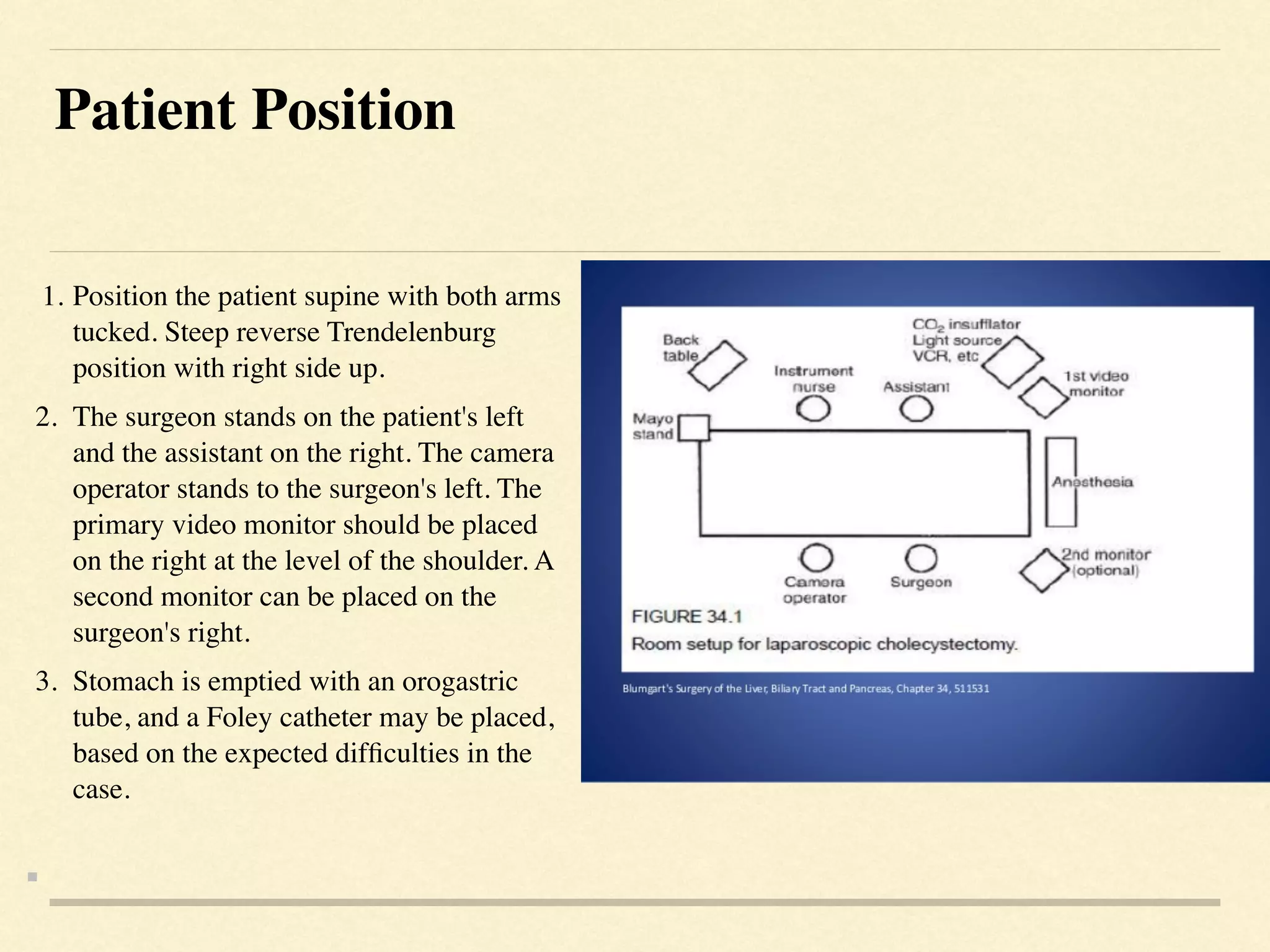

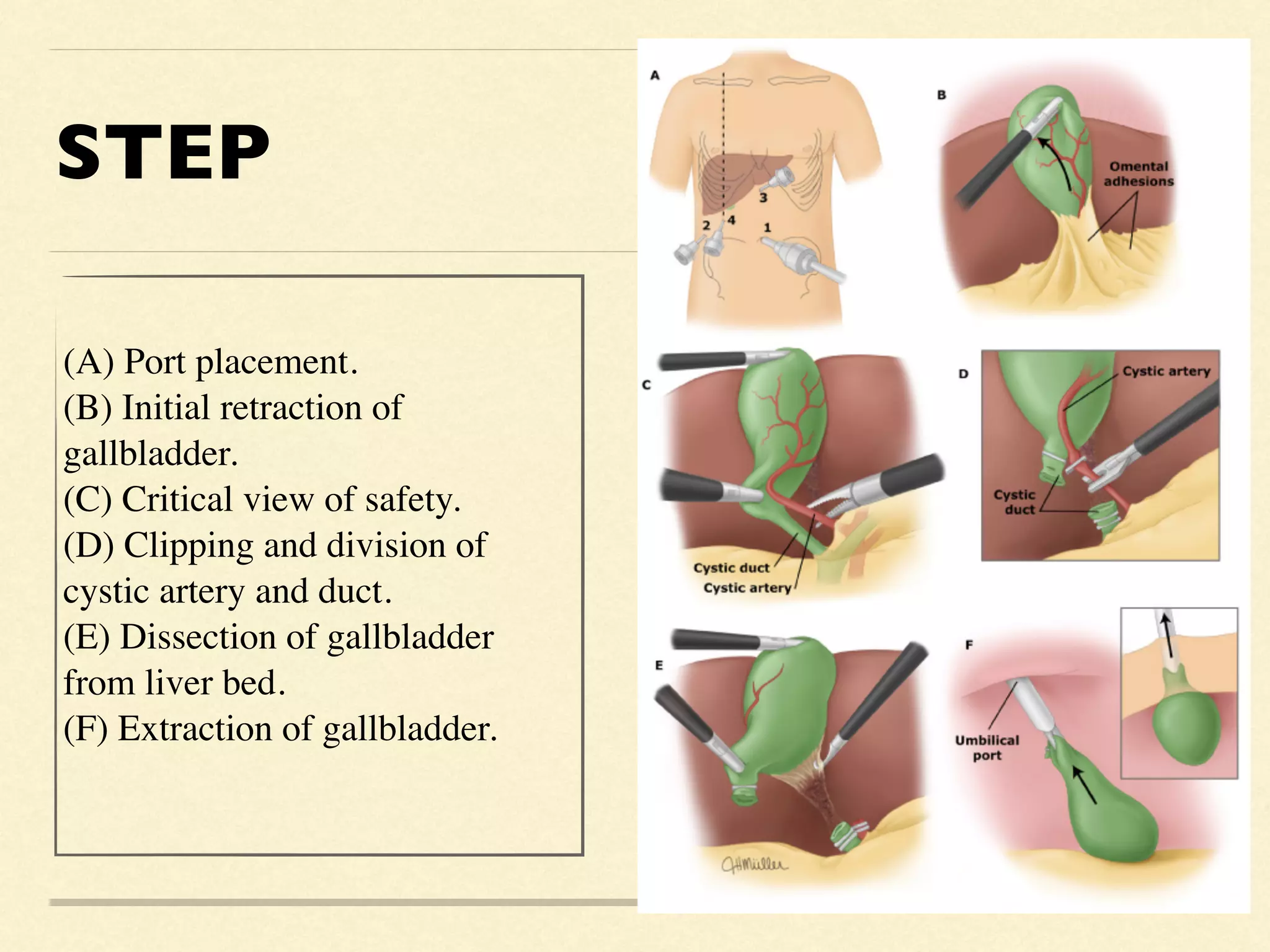




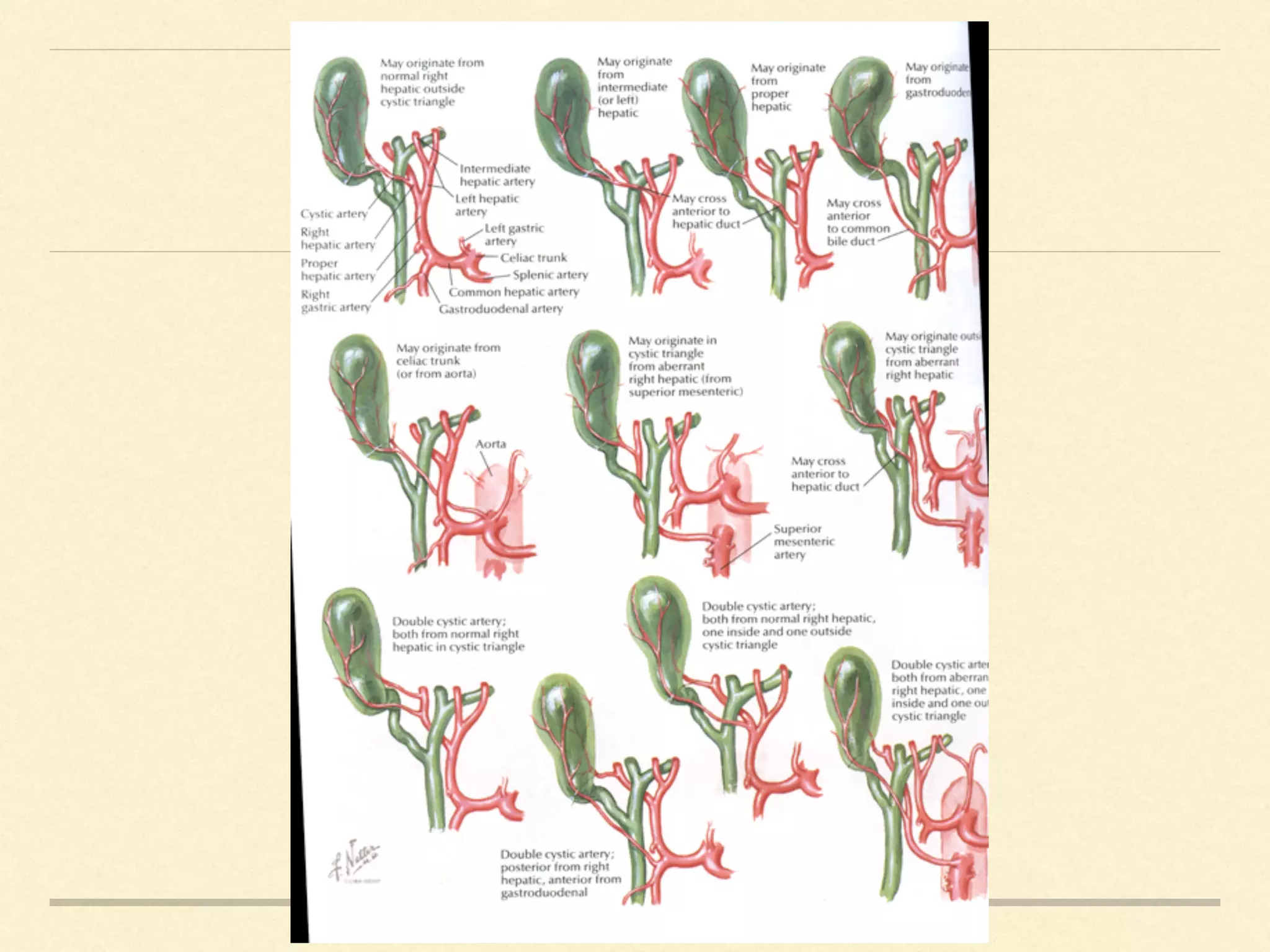



The document outlines essential techniques and tips for performing a safe laparoscopic cholecystectomy, emphasizing patient positioning, trocar placement, and the importance of the critical view of safety (CVS) during the procedure. It also highlights the necessity of recognizing aberrant anatomy, utilizing intraoperative cholangiography, and making safe surgical decisions in challenging conditions. Additionally, the document suggests enlisting help from another surgeon when dissection becomes difficult or hazardous.



































































