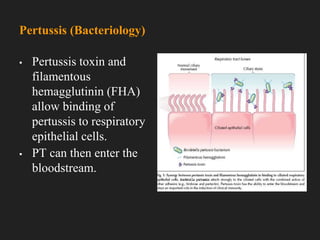
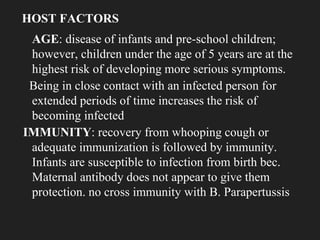
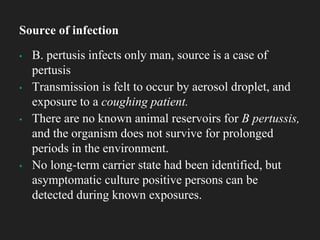
Whooping cough, or pertussis, is an acute infectious disease primarily affecting young children and caused by the bacterium Bordetella pertussis, which is highly contagious. The disease progresses through three stages: catarrhal, paroxysmal, and convalescent, with the characteristic 'whoop' often starting in the paroxysmal phase. Prevention includes vaccination, good hygiene practices, and antibiotics to interrupt transmission and treat symptomatic patients.




























![Bordetella pertusis ppt [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bordetellapertusispptautosaved-250119054438-6c19987e-thumbnail.jpg?width=640&height=640&fit=bounds)
![Bordetella pertusis ppt [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bordetellapertusispptautosaved-250119055602-ce139642-thumbnail.jpg?width=640&height=640&fit=bounds)














![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




