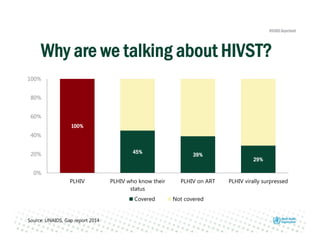
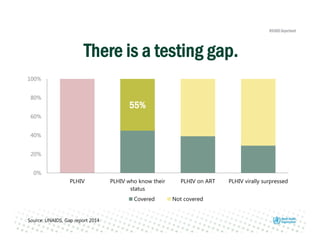
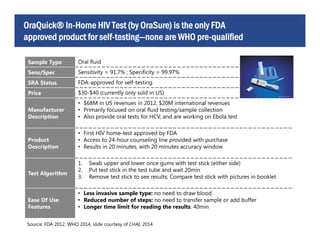
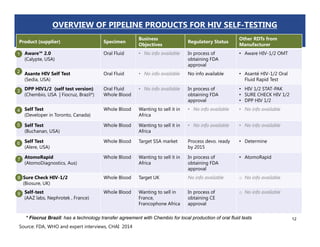
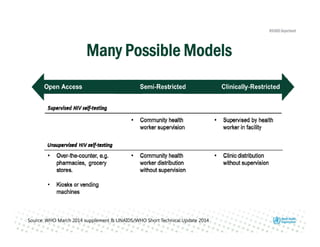
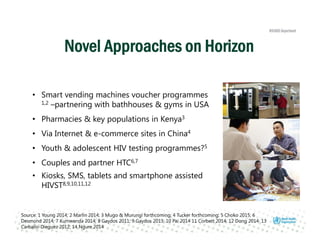
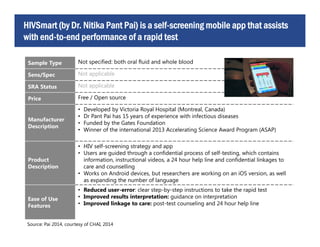
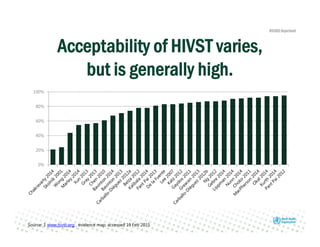
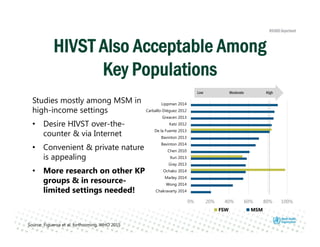
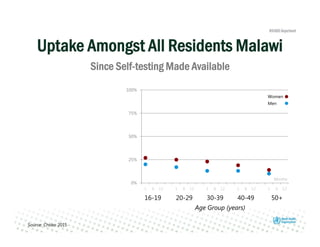
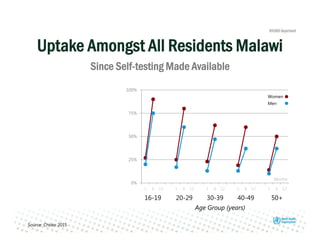
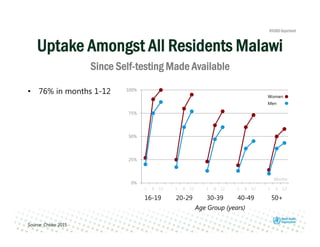
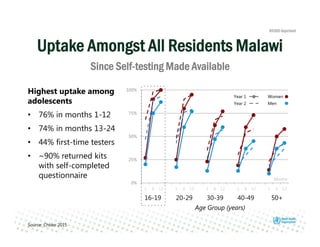
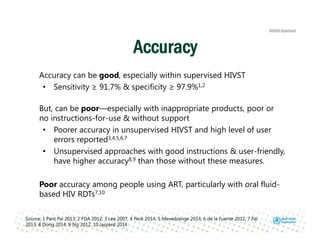
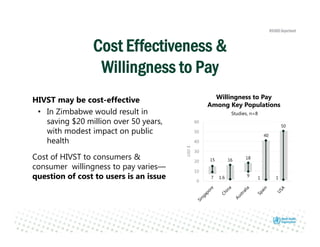
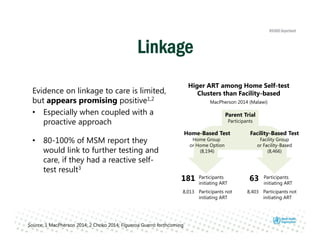
Rachel Baggaley presented an overview of HIV self-testing at the Bill and Melinda Gates Foundation meeting. There is a large testing gap, with only 45% of people living with HIV knowing their status. HIV self-testing could help close this gap by making testing more convenient and private. Several HIV self-testing products are in development using oral fluid or whole blood samples. Early evidence shows high acceptability of HIV self-testing, though accuracy can vary depending on how it is administered. Linkage to care also seems promising when self-testing is coupled with support services. More research is still needed on self-testing among key populations and in resource-limited settings.




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












