Download to read offline














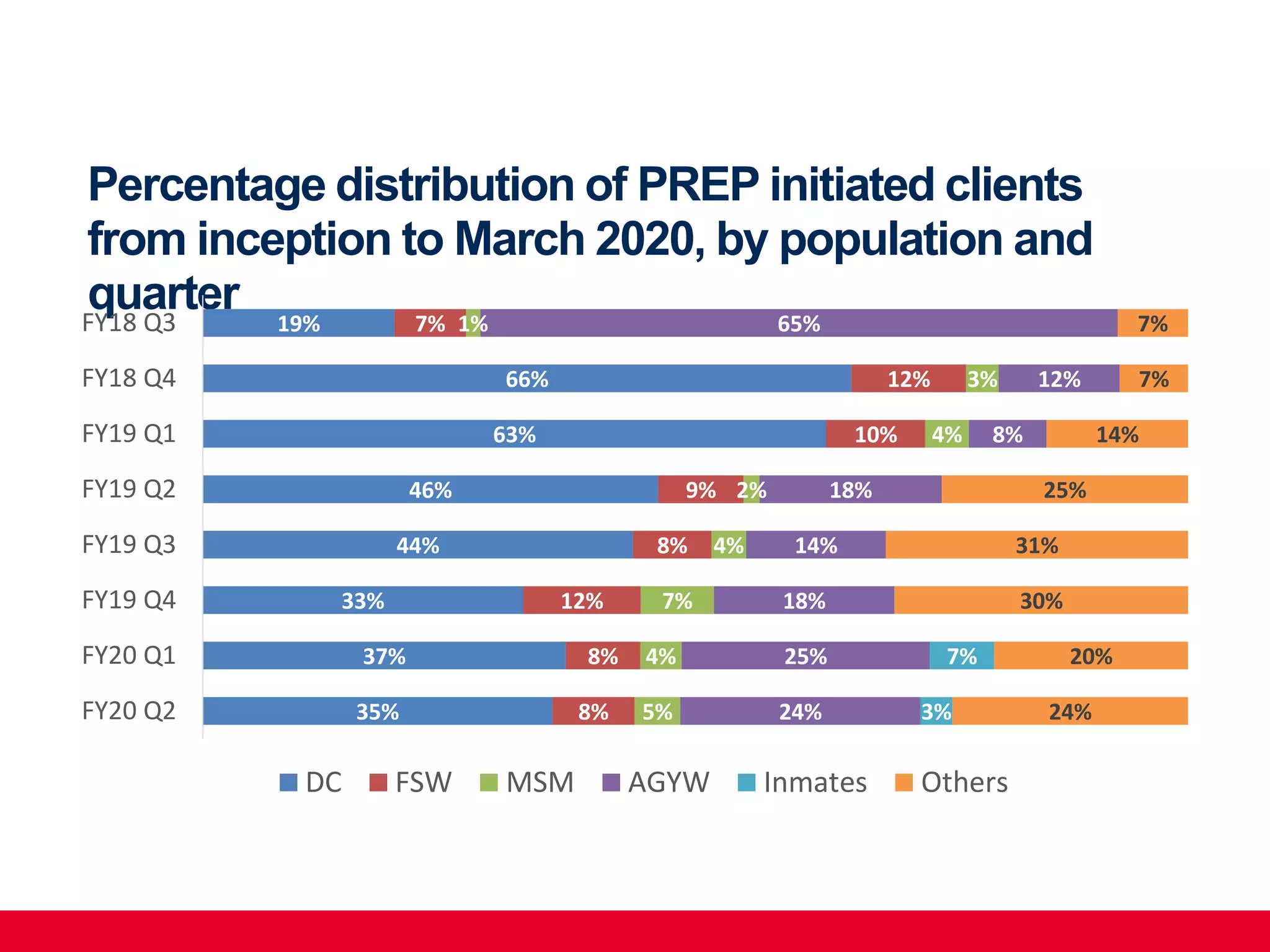
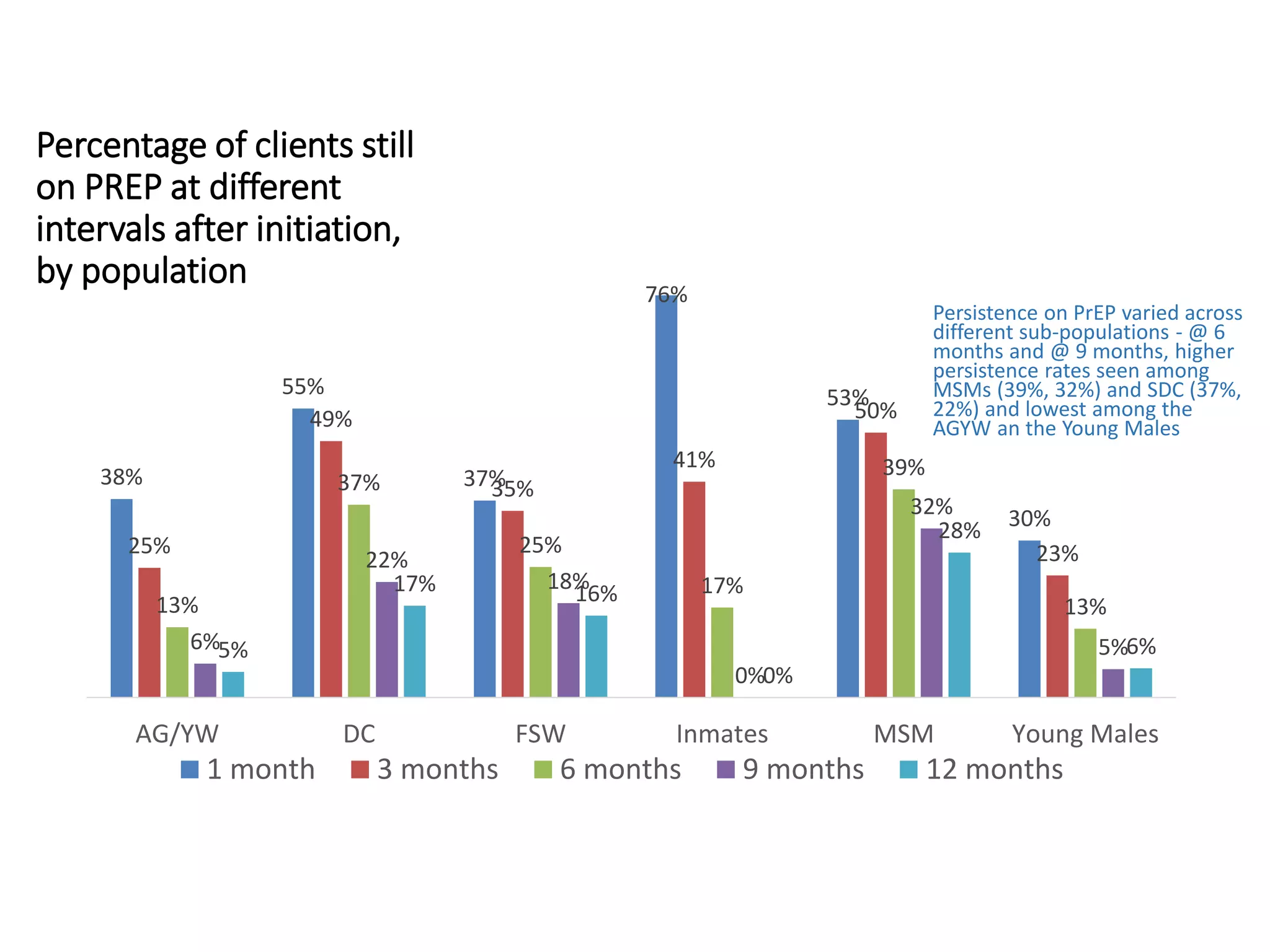





The document outlines a webinar discussing the management of Pre-Exposure Prophylaxis (PrEP) in various client scenarios, including young adults, pregnant individuals, and those with specific health conditions. It emphasizes the importance of adherence, counseling, and support for PrEP clients, and provides statistics on PrEP implementation in Zambia, including reasons for client discontinuation. Key recommendations include integrating PrEP with other health services and enhancing client engagement to address barriers to access.