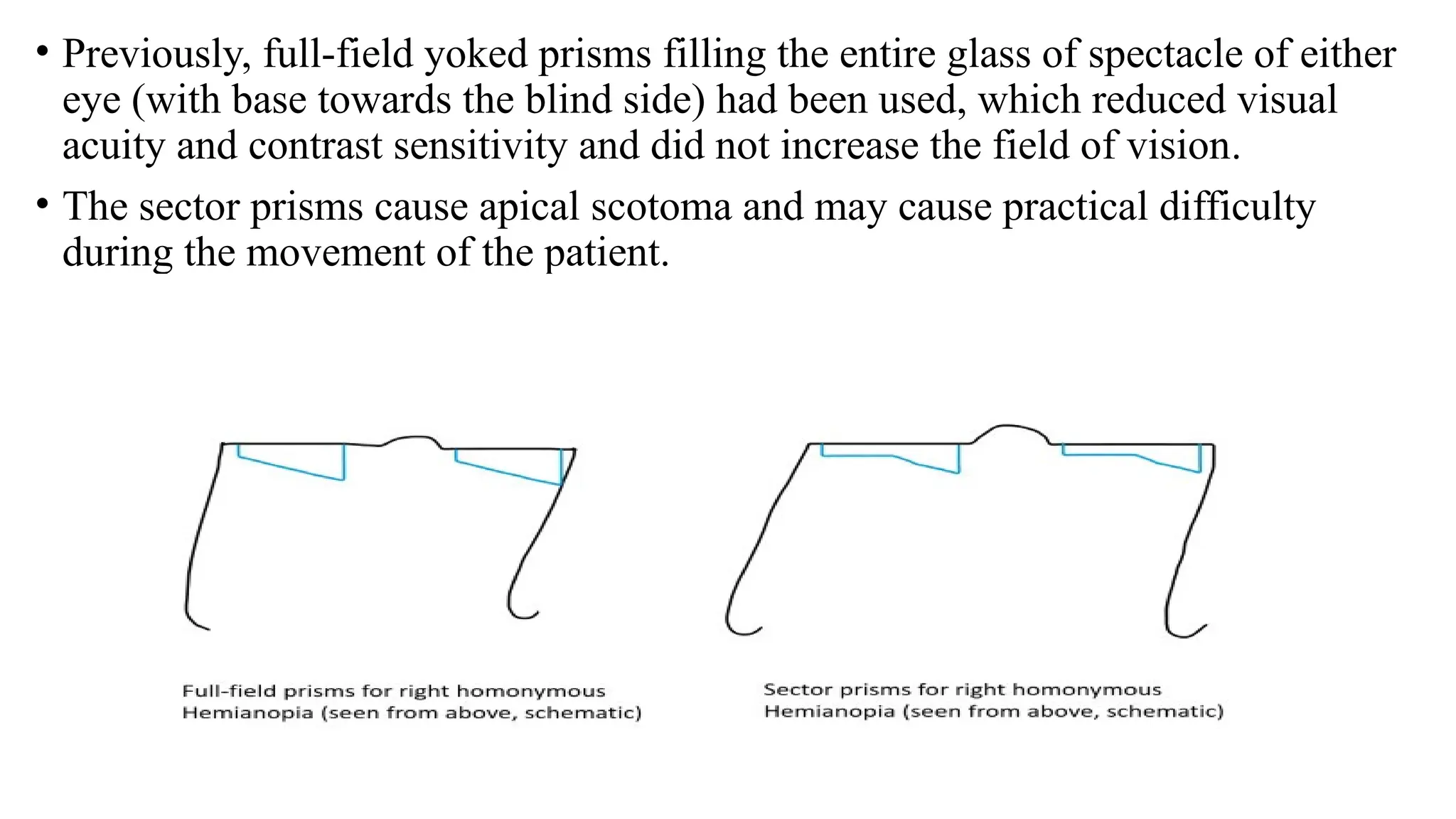
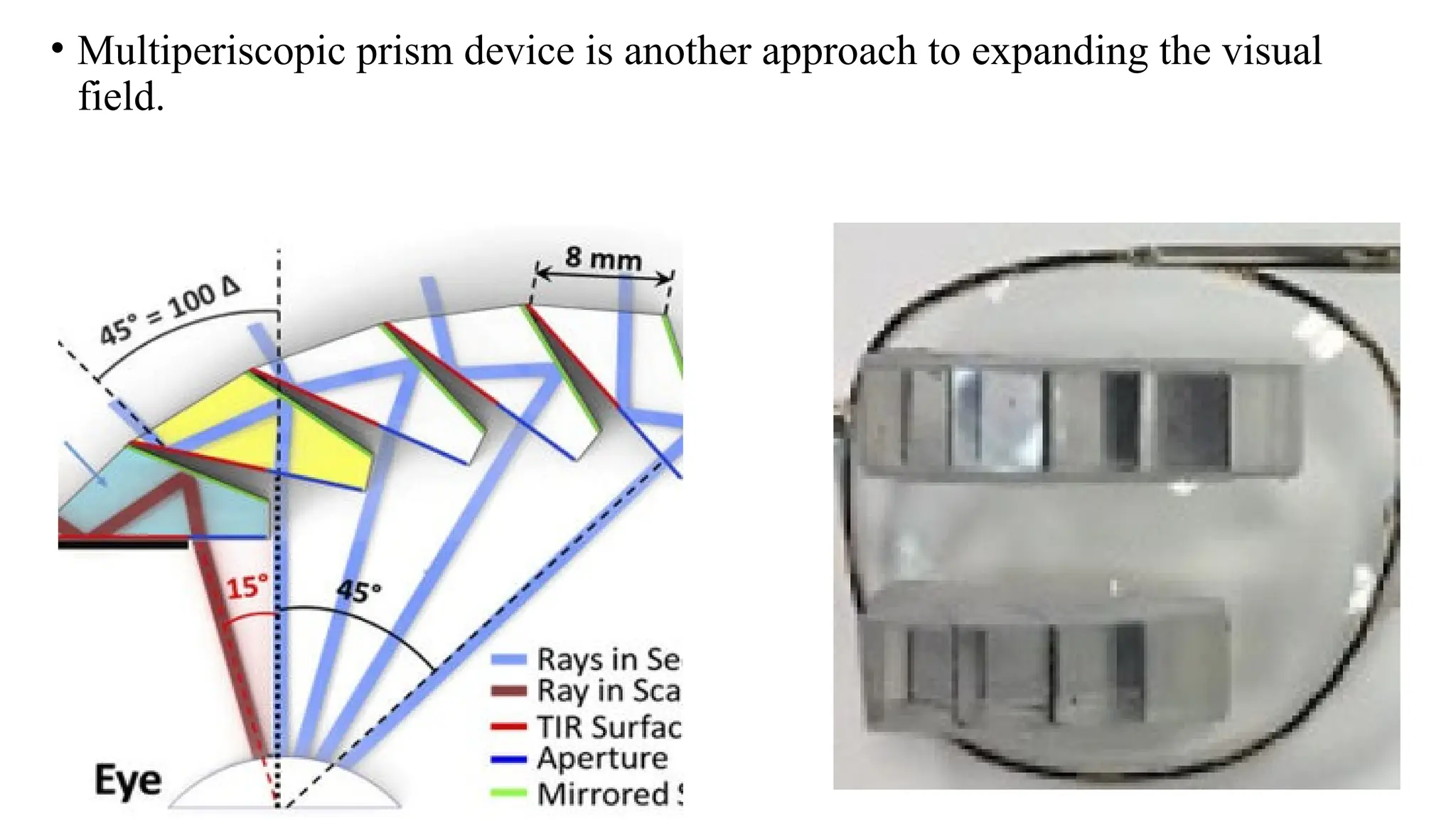
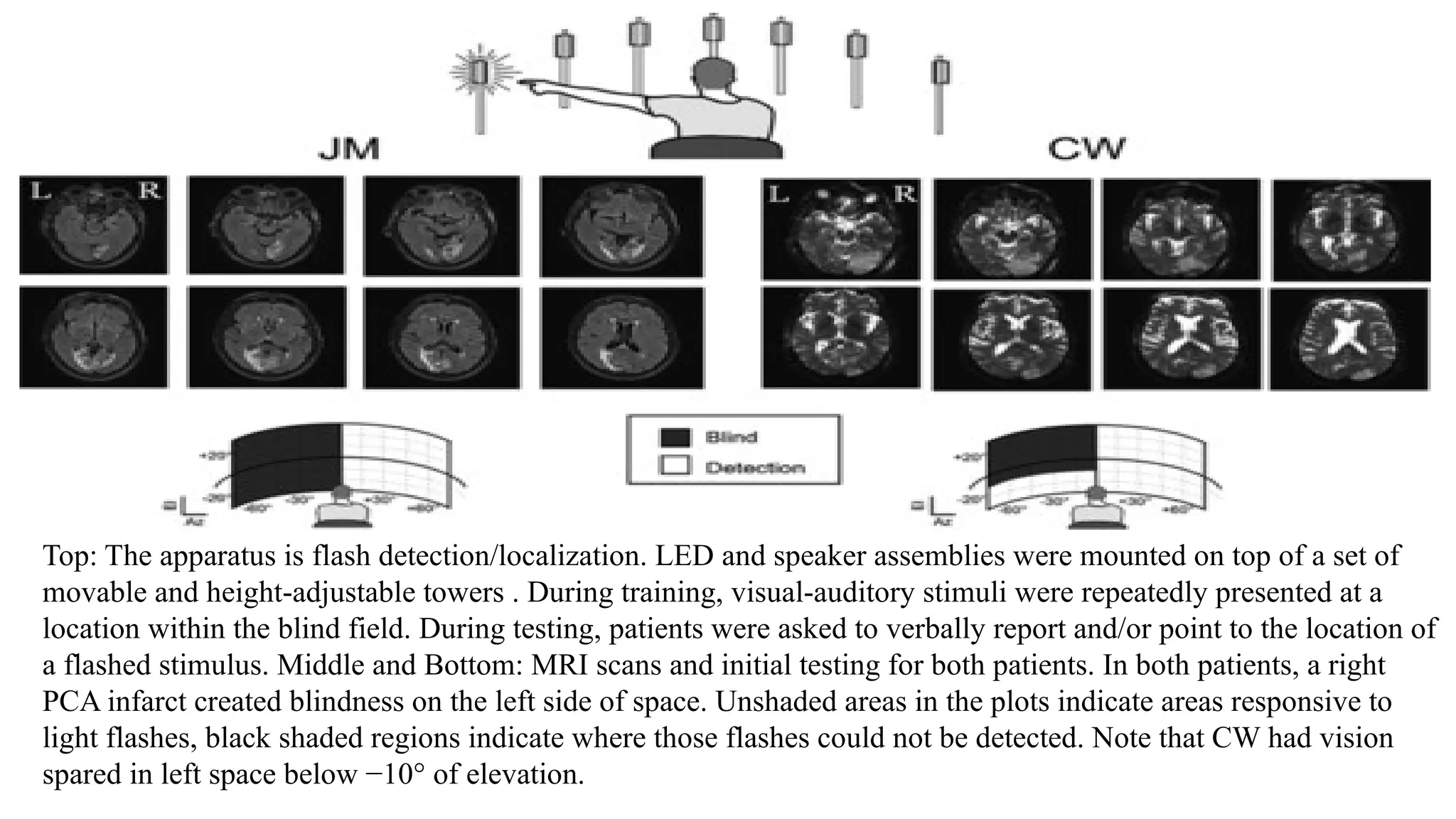
The document discusses hemianopia, a condition characterized by loss of vision in half of the visual field, detailing its causes, which include neurological disorders, stroke, and trauma, as well as the locations of lesions that lead to this condition. It addresses various treatment methods, including the use of Peli prisms to expand the visual field, multisensory therapy for improving visual function, and vision restoration therapy designed to help patients regain vision through structured exercises. Additionally, biofeedback training is mentioned as a modern rehabilitation technique that enhances visual acuity and quality of life for individuals with low vision.