Visual Cortex
Scientistsdiscovered
columns of neurons that
selectively respond to
visual information from
one eye or the other.
They learned that normal
visual experience during
a critical period in early
childhood is crucial for
these columns to form
properly
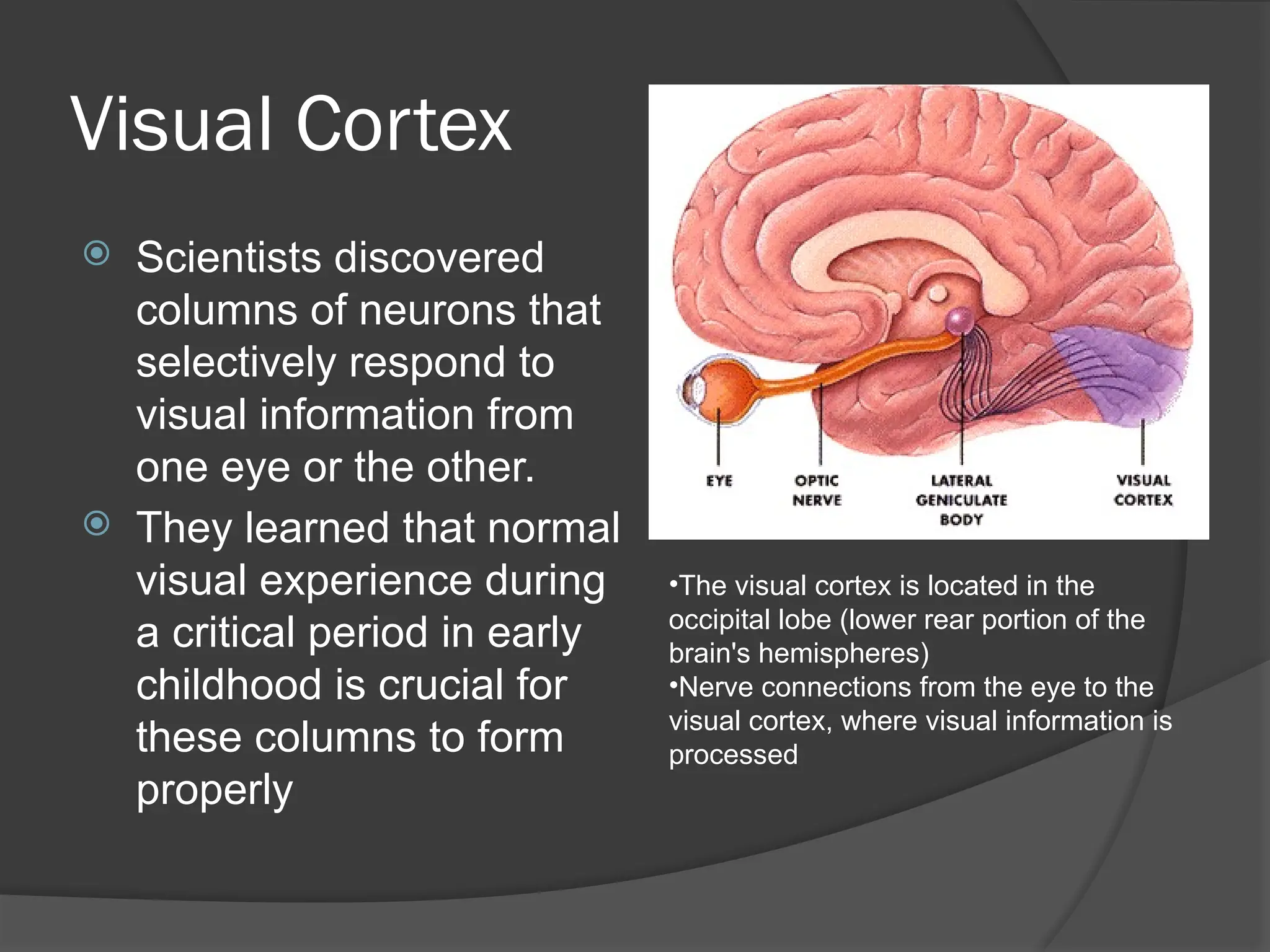
•The visual cortex is located in the
occipital lobe (lower rear portion of the
brain's hemispheres)
•Nerve connections from the eye to the
visual cortex, where visual information is
processed
3.
Physiology of thevisual pathway
The ability to focus a visual image on the
central retina develops at about two to three
months of age. Ideally, all rays of light
converge on the macula, the retinal area
where images can be most sharply
delineated.
Accommodation is the process by which the
ciliary body contracts, allowing the lens to
assume a greater curvature and to increase
refraction of light rays from near objects.
Accommodation is reflexively linked to
turning in of the eyes, or ocular convergence,
so that a binocular image is maintained.
4.
Physiology of thevisual pathway
When moving in unison, each eye focuses
the retinal image on its macula, and the
cortical image in the occipital brain is
reconciled into binocular "seeing." If the
retinal image is distorted in one eye because
of a refractive difference between eyes
(anisometropia) or a congenital cataract, or if
the visual axis misaligns the image on the
retina (strabismus), the cortical image is too
dissimilar to permit clear binocular resolution.
5.
Physiology of thevisual pathway
The brain quickly learns to suppress the poorer
image from the affected eye to allow for clear
vision. Since cortical visual development is
dependent on continuous stimuli,
neurodevelopment is impeded in the visual
cortex corresponding to the suppressed eye.
The result can be permanent visual impairment
(amblyopia) in an otherwise normal eye.
This process is dynamic and reverses if the
distortion of the retinal image is corrected; the
earlier the correction, the more likely full
development can be achieved.
6.
Normal Development
Acuityat birth is 6/120
Age 6 months V/A is 6/6
Color vision improves by 3 months
Eye color evolves by 9-12 months
Iris is lightest in color at birth
7.
Normal Visual Development
Visual acuity at birth is quite poor, typically
around 6/120. This is due to immaturity of the
central nervous system visual pathways and
visual processing areas.
Visual acuity improves to 6/30 by four months of
age, and this is the critical period of visual
development.
Visual acuity reaches nearly 6/6 by 12 months
of age, but special techniques are needed to
demonstrate it.
A cooperative 3-year old should demonstrate a
visual acuity of 6/12, and a 5-year old 6/9.
8.
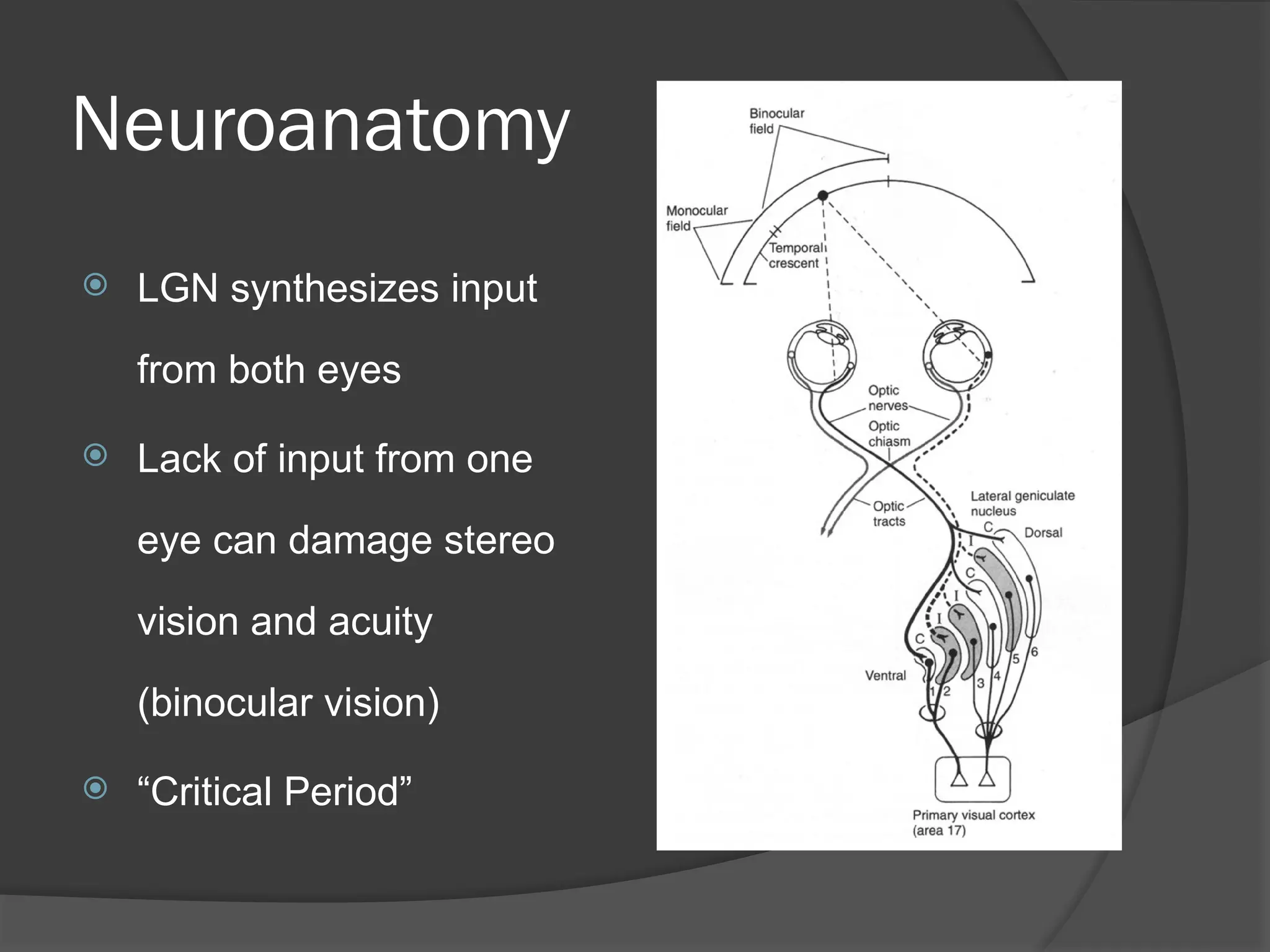
Neuroanatomy
LGN synthesizesinput
from both eyes
Lack of input from one
eye can damage stereo
vision and acuity
(binocular vision)
“Critical Period”
9.
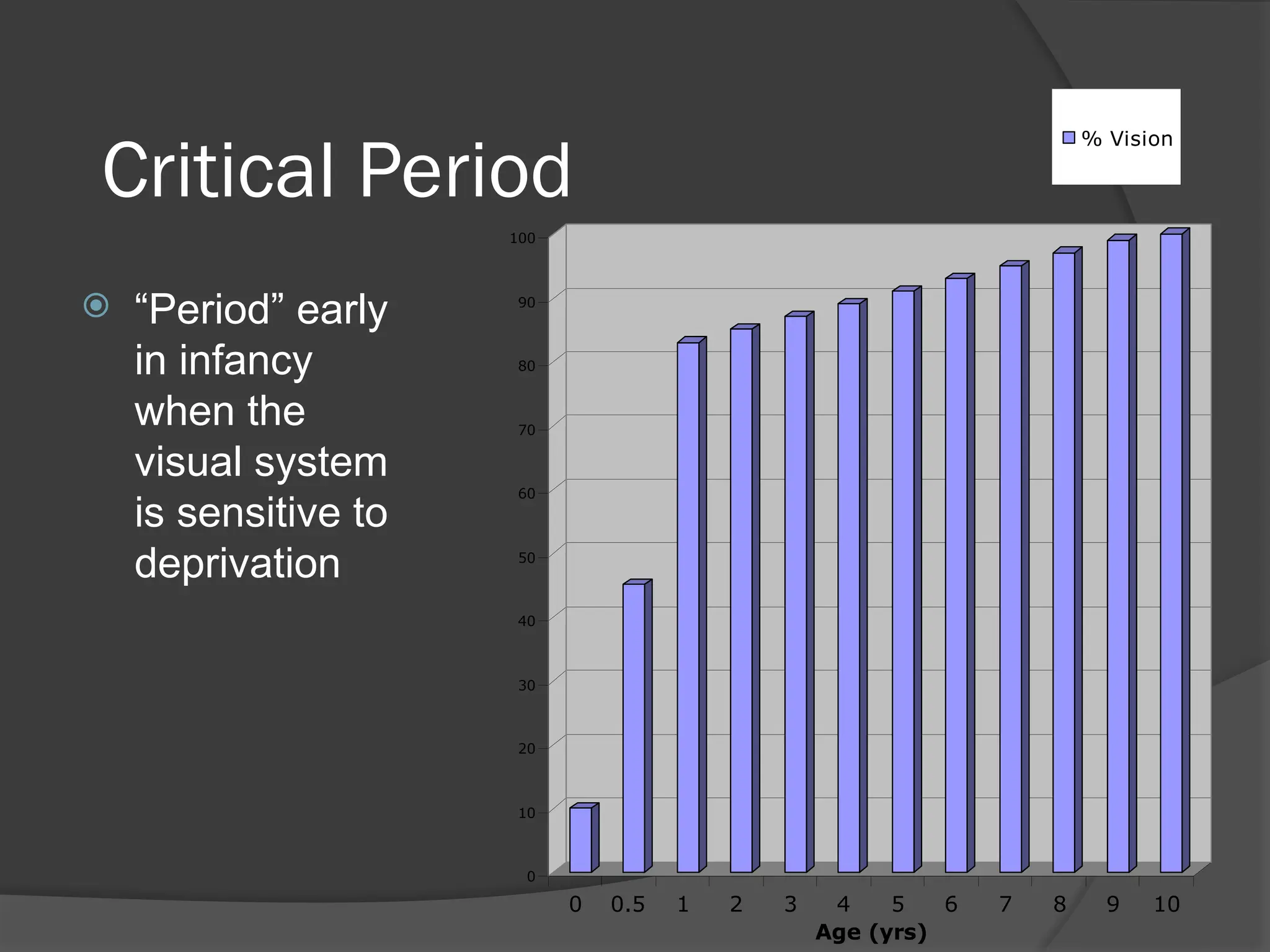
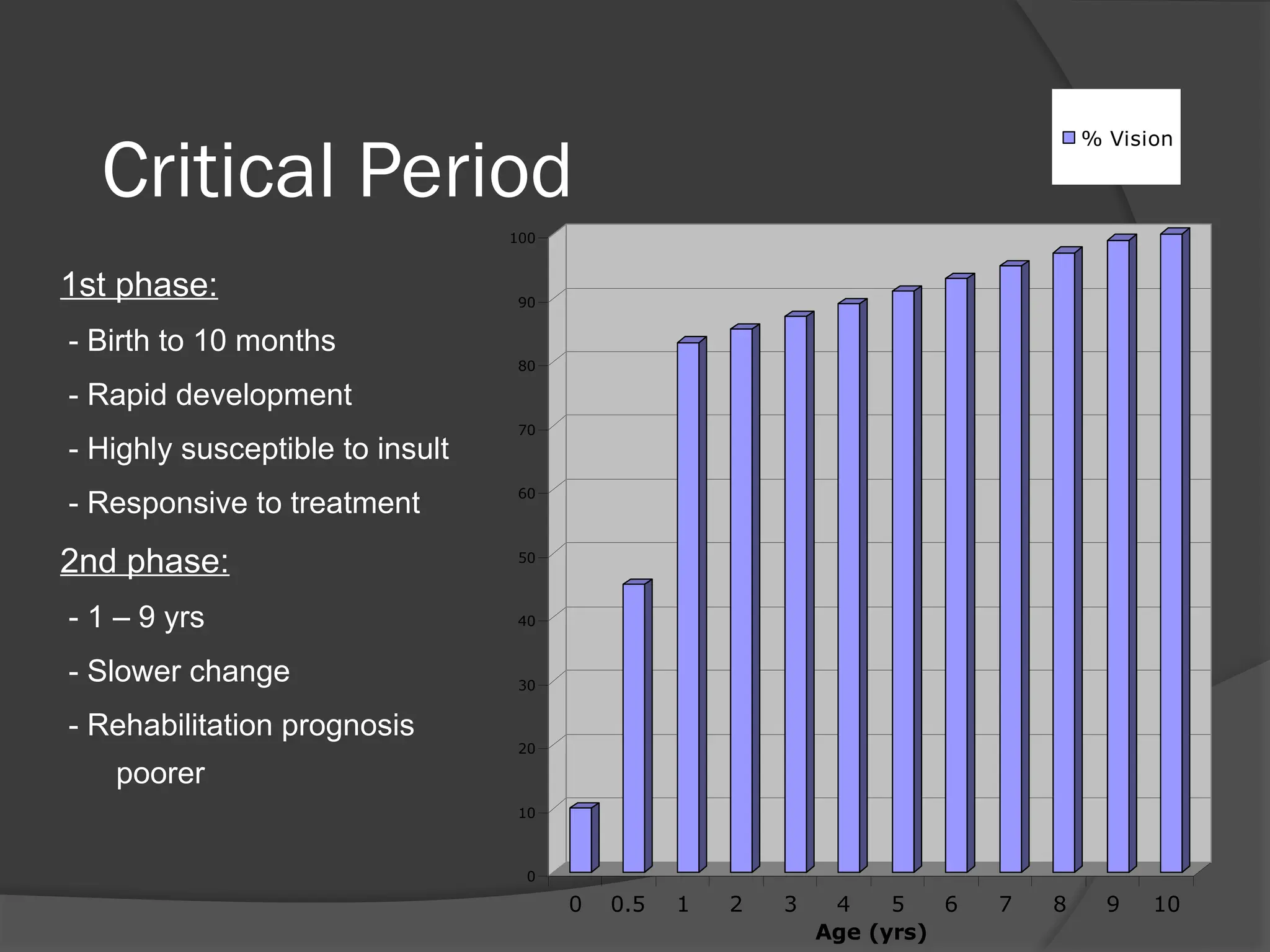
Critical Period
“Period”early
in infancy
when the
visual system
is sensitive to
deprivation
0
10
20
30
40
50
60
70
80
90
100
0 0.5 1 2 3 4 5 6 7 8 9 10
Age (yrs)
% Vision
Normal Visual Development
Many newborns show variable ocular alignment:
70% having exotropia (eye turns out) and
30% having straight eyes
Esotropia (eye turns in) is rare.
By 2 - 3 months of age, most infants will have
straight eyes.
Misaligned eyes beyond 3 months of age
require ophthalmic evaluation
12.
Schedule of RecommendedPediatric
Vision Screening Based on Patient Age
Neonate
External (penlight) examination for surface
abnormalities of the eye and surrounding
tissues
Ocular alignment (corneal reflections)
Ophthalmoscopy for red reflexes
13.
Schedule of RecommendedPediatric
Vision Screening Based on Patient Age
Age six months
Ability to fix and follow light, face or small toy
External (penlight) examination for surface
abnormalities of the eye and surrounding
tissues
Pupillary examination
Ocular alignment (corneal reflections)
Ophthalmoscopy for red reflexes
14.
Schedule of RecommendedPediatric
Vision Screening Based on Patient Age
Age 3 - 4 years
Visual acuity by picture chart or tumbling E chart
External (penlight) examination for surface
abnormalities of the eye and surrounding tissues
Pupillary examination
Ocular motility and alignment (ocular
movements, cover test and corneal reflections)
Ophthalmoscopy for red reflexes and
examination of retina and optic nerve
15.
Schedule of RecommendedPediatric
Vision Screening Based on Patient Age
Age 5 - 6 years
Visual acuity by Snellen method
External (penlight) examination for surface
abnormalities of the eye and surrounding tissues
Pupillary examination
Ocular motility and alignment (ocular
movements, cover test and corneal reflections)
Ophthalmoscopy for red reflexes and
examination of retina and optic nerve