Downloaded 16 times


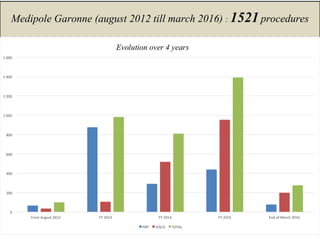

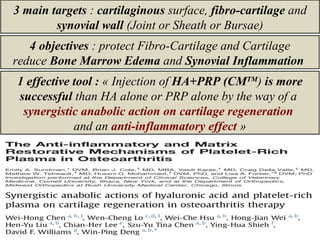


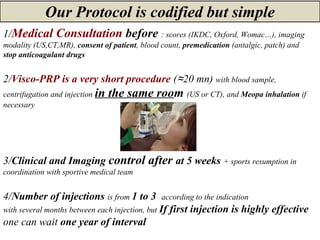
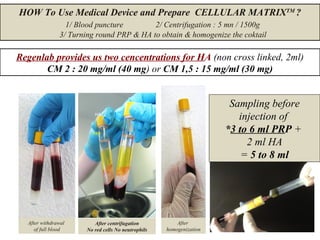









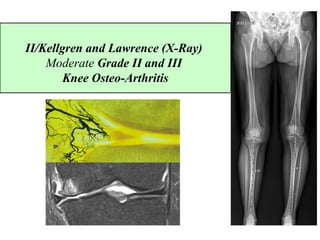


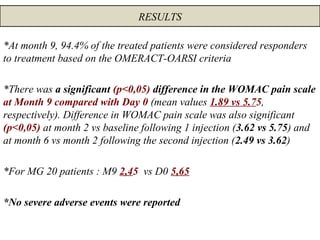
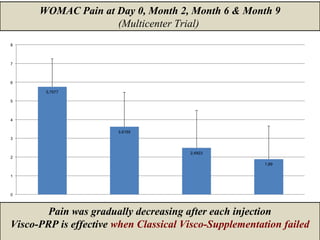






























1) Cellular Matrix is an all-in-one injection of hyaluronic acid and platelet-rich plasma for fibrocartilaginous tears, osteoarthritis, and bone marrow lesions. 2) A study of over 1500 procedures found Cellular Matrix injections to be effective for lower limb issues like the knee in 92.8% of cases. 3) A trial of 71 patients with knee osteoarthritis who had previously failed hyaluronic acid treatment found significant pain reduction and a 94.4% response rate following Cellular Matrix injections, indicating it may be effective when other treatments have failed.















































































