INFLAMMATION/INFECTION
• Medical terminologyreflects site
• Cellulitis
• Myositis
• Vasculitis
• May be inflammatory or infectious
• diffuse (cellulitis/infectious cellulitis)
• focal (seroma/abscess)
• May be life threatening
• Therapy
• Anti-inflammatory agents: NSAID, topical DMSO
• Hot pack
• +/- antibiotics
4.
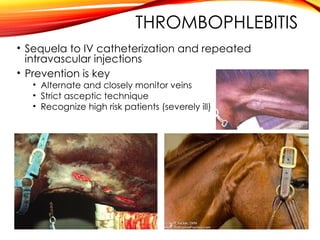
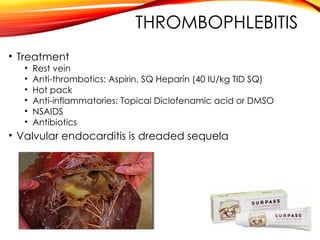
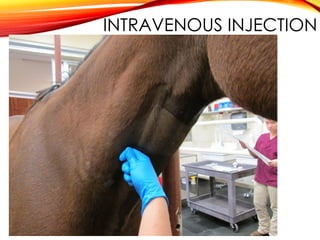
THROMBOPHLEBITIS
• Sequela toIV catheterization and repeated
intravascular injections
• Prevention is key
• Alternate and closely monitor veins
• Strict asceptic technique
• Recognize high risk patients (severely ill)
INJECTION ABSCESS
• Findsource
• Culture?
• Therapy
• Lance, drain, and lavage if possible
• Anti-inflammatories : NSAID, topical DMSO
• Hot pack if can’t be drained
• Antibiotics will compromise ability to drain
abscess but are indicated if anorexic, febrile
and abscess can’t be drained or impinges vital
structures
14.
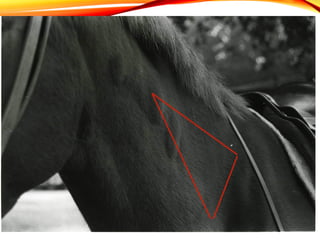
INTRARRHACHIDIAN
CERVICAL INJECTION
• Injectionbetween cervical vertebrae that
penetrates meninges (intraspinal)
• History is critical
• Sequelae to incorrect IM injection in neck
• Clinical Signs: referrable to NECK PAIN
• Reluctant to move
• Won’t lower head to eat
• improperly called anorexia
• Forelimb lameness
• usually unilateral on side of injection
• Pyrexia
• Heat/pain/swelling at injection site are variable
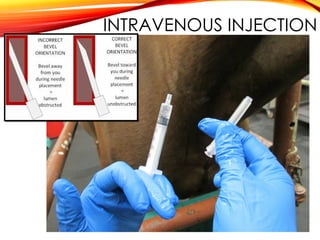
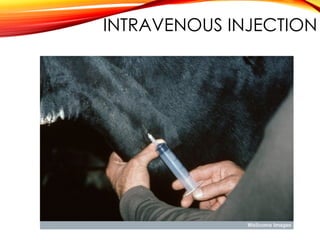
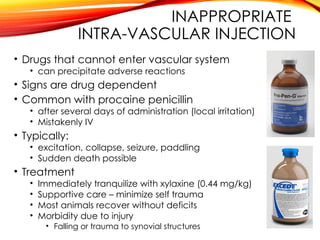
INAPPROPRIATE
INTRA-VASCULAR INJECTION
• Drugsthat cannot enter vascular system
• can precipitate adverse reactions
• Signs are drug dependent
• Common with procaine penicillin
• after several days of administration (local irritation)
• Mistakenly IV
• Typically:
• excitation, collapse, seizure, paddling
• Sudden death possible
• Treatment
• Immediately tranquilize with xylaxine (0.44 mg/kg)
• Supportive care – minimize self trauma
• Most animals recover without deficits
• Morbidity due to injury
• Falling or trauma to synovial structures
28.
EXTRAVASCULAR
LEAKAGE
• Extravascular (perivascular)drug deposition
• Causes local irritation and tissue necrosis
• Can take several days to fully develop
• Phenylbutazone is most common
• Drugs with High or low pH more likely to irritate
• Prevention is key!!!
• Re-evaluate needle placement frequently
• During injection and if animal moves
• Treatment: ‘dilution is the solution to pollution’
• Locally infiltrate area with saline (10-15mL)
• +/- dexamethasone, procaine penicillin
• Hot pack
• Consider ventral drainage if large volume perivascular
29.
HYPERSENSITIVITY
• State ofexcessive reactivity to an antigen
• Allergy often used as synonym
• Outcome is deleterious rather than protective
• Gell and Coombs Classification:
• 4 main types of hypersensitivity (I-IV)
• Classification based on:
• nature of inflammatory response
• tissue damage
• Covered in depth next semester
30.
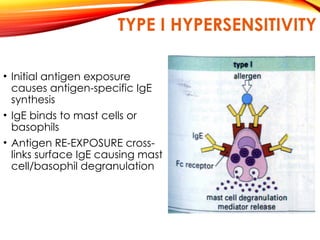
TYPE I HYPERSENSITIVITY
•Initial antigen exposure
causes antigen-specific IgE
synthesis
• IgE binds to mast cells or
basophils
• Antigen RE-EXPOSURE cross-
links surface IgE causing mast
cell/basophil degranulation
31.
INFLAMMATORY MEDIATORS
Three Sources:
1.Released from mast cell granules
2. Synthesized upon degranulation
3. Brought in: from chemo-attracted cells
Commonly Cited Mediators:
-Histamine
-Cytokines: TNF, IL-4, IL-5, IL-8, IL-13
-Prostaglandins
-Leukotrienes
-Enzymes
-In reality there are hundreds characterized to date
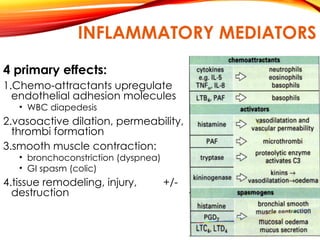
INFLAMMATORY MEDIATOR
EFFECTS
•Mediators havedefined physiologic effects
•Clinical outcome of type I reactions depends upon
•Characteristics of individual
• amount of IgE present
• Individual responsiveness to mediators (varies)
•Characteristics of allergen
• dose
• potency
•Site of allergen introduction and degree of
dissemination
• SYSTEMIC
• LOCALIZED
35.
PHYSIOLOGIC EFFECT OF
MEDIATORS
•DirectAg introduction to blood or rapid absorption
widespread activation of connective tissue mast
cells in vessels and systemic anaphylaxis
•Ag inhalation
upper respiratory: rhinitis
lower respiratory: recurrent airway obstruction
•Skin
Localized injection- wheal and flare
Disseminated from GI absorption: urticaria
38.
PHYSIOLOGIC EFFECT OF
MEDIATORS
1.Vasodilation
•Localized: erythema
• Systemic: hypotension
2.Capillary damage
• Thrombi
• Increased permeability Edema
…signs are site dependent!
• Skin: urticaria
• GI: Diarrhea, Gastric distention and pain
(horses can’t vomit)
• Upper respiratory tract : Dyspnea
• Systemic: Hemoconcentration, Hypoproteinemia
….continued on next slide
TYPE I EQUINE
HYPERSENSITIVITY
Exactrole of IgE mediated hypersensitivity in horses
becomes sketchy:
• reagents for equine IgE research have limited availability
• Systemic anaphylaxis
• Many urticarial reactions
• Local anaphylaxis
• Insect and parasite hypersensitivities
• Atopic dermatitis
• Feed Hypersensitivity
• Respiratory manifestations
• Atopic respiratory disease
• Inflammatory Airway disease
• Recurrent Airway obstruction
41.
SYSTEMIC ANAPHYLAXIS
(FAIRLY COMMON)
•Anaphylactic Shock
• Onset within 30 min of Ag exposure
(hours if Ag is metabolite)
• Immunologic vs Non-immunologic triggering
• Most common antigens are biologics:
• Sera, vaccines (IgE-Driven)
• Therapeutics less common
• small simple molecules
• Often via direct activation of Complement-kinin system
• Structurally related compounds can cross react
• Disease can be localized or systemic
• Localized reaction can progress to life threatening
systemic RXN
42.
SYSTEMIC ANAPHYLAXIS
• Anydrug, via any route, at any time
• Longer duration, higher dose increases risk
• Atopic individuals higher risk (IL-4, IL-13/Th2)
• Examples:
• thiamine, vitamin E, Selenium
• anthelmintics
• penicillin, TMS, chloramphenicol, aminoglycosides,
tetracyclines
• halothane, guaifenesin
ANAPHYLAXIS
• Differentials:
• Druginteractions
• Inappropriate route
• Others specific to signs demonstrated
• Colic differentials
• Respiratory disease
• Other (uriticaria differentials…etc)
• Diagnostics
• Signs and history
• CBC and serum biochemistries are variable
• ECG: can develop signs of hypoxemia
• prolonged QRS, ST depression
45.
TREATMENT
EARLY INTERVENTION ISKEY
• Not all reactions require therapy
• Sudden Dyspnea and hypotension warrant aggressive
therapy
• monitor less severe reactions closely
• Goals:
• counteract mediators
• maintain respiratory and CV stability
46.
TREATMENT
• Remove antigen!!!!
•Place IV catheter
• Assure airway – tracheotomy may be required
• GLUCOCORTICOIDS *hallmark of Rx*
• Prednisolone sodium succinate
• 0.25-1.0 mg/kg
• IV fluids: shock volumes
• Oxygen
• Cardiac monitoring
• Epinephrine…with caution
• Antihistamines, NSAIDS
47.
EPINEPHRINE THERAPY
IN HORSES
•Why? sympathetic stimulant: α1, α2, β 1, β2
• KNOW how the drugs work
• Excitement
• IV admin to standing horse is ill advised
• IM (10-20 ug/kg = 5-10 ml of 1:1000)
• If dyspnea or hypotension are mild
• IV (3-5 ug/kg = 1.5-2.25 ml of 1:1000)
• If severe dyspnea or hypotension
• Endotracheal if no venous access
• Repeat every 15 minutes until hypotension improves
• Refractory cases may need epinephrine or
norepinephrine CRI
#41 Can be activation of IgE (larger molecules, previous sensitization) or- direct activation of complement-kinin system by some part of the drug (usually smaller molecules)

































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
