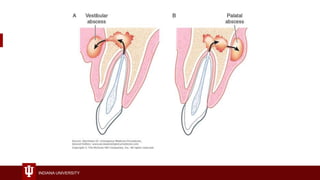
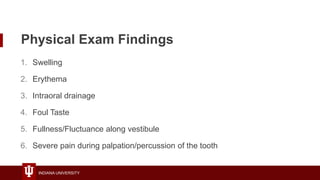
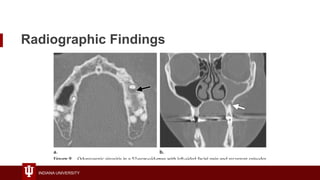
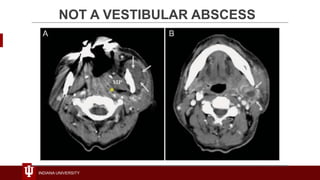
This document discusses dental vestibular abscesses and their drainage. It covers common causes of abscesses like infected cysts or gingival infections. It describes the anatomy and signs of a vestibular abscess like swelling, erythema and pain. The document provides guidance on properly examining, preparing and performing an incision and drainage of a vestibular abscess intraorally using local anesthesia and a blade. Potential complications are minor pain, swelling and bleeding.