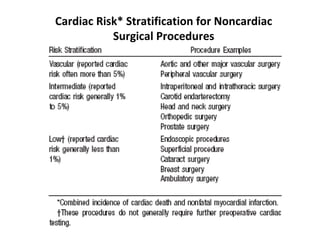
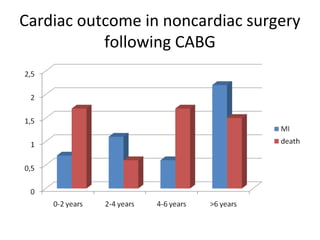
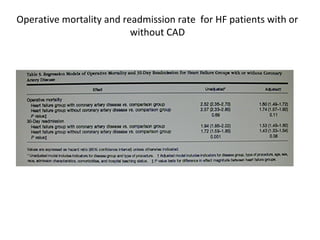
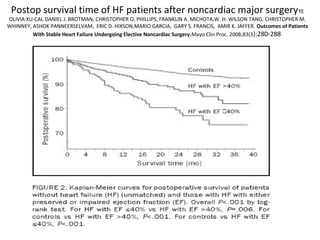
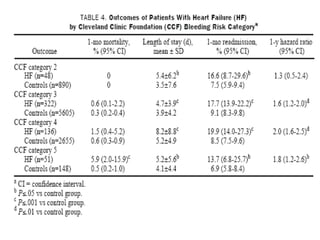
The document discusses the preoperative cardiac risk assessment for patients undergoing noncardiac surgery, emphasizing the importance of accurately predicting perioperative events and the need for appropriate risk stratification tools. It highlights various clinical factors affecting cardiac risk, such as age, specific medical conditions, and exercise tolerance, along with recommendations for evaluation and management before surgery. Additionally, it underscores that unnecessary interventions to merely reduce surgical risk should be avoided unless indicated by the patient's condition.
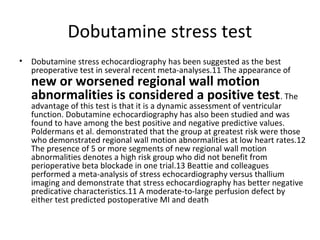
![Anesthesiology. 2004 Aug;101(2):284-93.Effect of clonidine on
cardiovascular morbidity and mortality after noncardiac surgery.
Wallace AW, Galindez D, Salahieh A, Layug EL, Lazo EA, Haratonik KA,
Boisvert DM, Kardatzke D.
• Department of Anesthesia and Perioperative Care, University of California, USA.
awallace@cardiacengineering.com
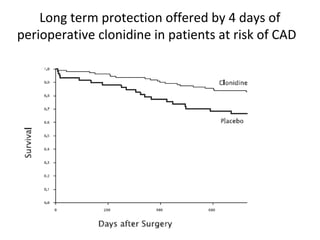
• BACKGROUND: Perioperative myocardial ischemia occurs in 20-40% of patients at risk for cardiac
morbidity and is associated with a ninefold increase in risk of cardiac morbidity. METHODS: In a
prospective, double-blinded, clinical trial, we studied 190 patients with or at risk for coronary artery
disease in two study groups with a 2:1 ratio (clonidine, n = 125 vs. placebo, n = 65) to test the
hypothesis that prophylactic clonidine reduces the incidence of perioperative myocardial ischemia and
postoperative death in patients undergoing noncardiac surgery. Clonidine (0.2 mg orally as well as a
patch) or placebo (tablet and patch) was administered the night before surgery, and clonidine (0.2 mg
orally) or placebo (tablet) was administered on the morning of surgery. The patch or placebo remained
on the patient for 4 days and was then removed. RESULTS: The incidence of perioperative myocardial
ischemia was significantly reduced with clonidine (intraoperative and postoperative, 18 of 125, 14%
vs. placebo, 20 of 65, 31%; P = 0.01). Prophylactic clonidine administration had minimal hemodynamic
effects. Clonidine reduced the incidence of postoperative mortality for up to 2 yr (clonidine, 19 of 125
[15%] vs. placebo, 19 of 65 [29%]; relative risk = 0.43 [confidence interval, 0.21-0.89]; P = 0.035).
CONCLUSIONS: Perioperative administration of clonidine for 4 days to patients at risk for coronary
artery disease significantly reduces the incidence of perioperative myocardial ischemia and
postoperative death.](https://image.slidesharecdn.com/valutazrischioanestsianapolidic2008-141222045855-conversion-gate01/85/Valut-az-rischio-anest-sia-napoli-dic-2008-italian-bibliografy-59-320.jpg)
![• Am J Med. 2009 Jan 28. [Epub ahead of print]
Links
• Perioperative Beta-blockers for Major
Noncardiac Surgery: Primum Non Nocere.
• Chopra V, Plaisance B, Cavusoglu E,
Flanders SA, Eagle KA.
• Division of General Medicine, Department of
Internal Medicine, University of Michigan
Health System, Ann Arbor.](https://image.slidesharecdn.com/valutazrischioanestsianapolidic2008-141222045855-conversion-gate01/85/Valut-az-rischio-anest-sia-napoli-dic-2008-italian-bibliografy-62-320.jpg)


![.N-TERMINAL PRO-BRAIN NATRIURETIC PEPTIDE
.ENDOGENOUS NITRIC OXIDE SYNTHASE INHIBITOR
ASYMMETRIC DIMETHYLARGININE
. POLYMORPHISMS IN PLATELET GLYCOPROTEIN
(GP) IIIA AND GPIB[ALPHA]
Laboratory markers for cardiac risk
after noncardiac surgery](https://image.slidesharecdn.com/valutazrischioanestsianapolidic2008-141222045855-conversion-gate01/85/Valut-az-rischio-anest-sia-napoli-dic-2008-italian-bibliografy-89-320.jpg)
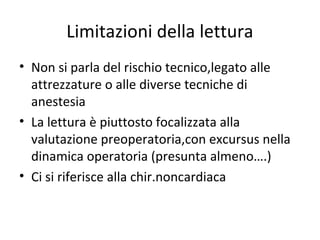
![Laboratory markers for cardiac risk after noncardiac surgery
• Elevated NT-proBNP levels are independently associated with an increase in the risk
of perioperative cardiovascular KO
– Yun KH, Jeong MH, Oh SK, Choi JH, Rhee SJ, Park EM, Yoo NJ, Kim NH, Ahn YK, Jeong JW.Preoperative plasma N-terminal pro-brain natriuretic
peptide concentration and perioperative cardiovascular risk in elderly patients.Circ J.2008 Feb;72(2):195-9.
– Leibowitz D, Planer D, Rott D, Elitzur Y, Chajek-Shaul T, Weiss ATBrain natriuretic peptide levels predict
perioperative events in cardiac patients undergoing noncardiac surgery: a prospective study.
Cardiology. 2008;110(4):266-70. Epub 2007 Dec 12.
• per 0.1-micromol/L increment in plasma ADMA
concentration, the odds ratio to experience the
primary end point increased by 1.26
– Maas R, Dentz L, Schwedhelm E, Thoms W, Kuss O, Hiltmeyer N, Haddad M, Klöss T, Standl T, Böger RH.Elevated plasma concentrations of the
endogenous nitric oxide synthase inhibitor asymmetric dimethylarginine predict adverse events in patients undergoing noncardiac surgery. Crit
Care Med. 2007 Aug;35(8):1876-81
• Polymorphisms in platelet glycoprotein (GP) IIIa and
GPIb[alpha]. Pro33 and Met145 genotypes were
independent predictors of composite ischemic
outcome
– Faraday, Nauder , Martinez, Elizabeth A. Scharpf, Robert B. Kasch-Semenza, Laura ; Dorman, Todd ; Pronovost, Peter J.
Perler, Bruce ; Gerstenblith, Gary Bray, Paul F. Fleisher, Lee A. Platelet Gene Polymorphisms and Cardiac Risk Assessment
in Vascular Surgical Patients. Anesthesiology. 101(6):1291-1297, December 2004.](https://image.slidesharecdn.com/valutazrischioanestsianapolidic2008-141222045855-conversion-gate01/85/Valut-az-rischio-anest-sia-napoli-dic-2008-italian-bibliografy-90-320.jpg)













![Chapter 2 pre_anesthetic_evaluation_presentation_1_for_students [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter2preanestheticevaluationpresentation1forstudentsautosaved-210422073416-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















