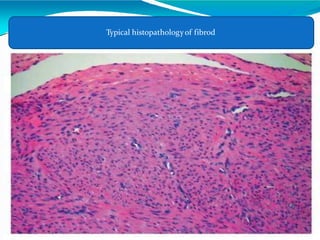
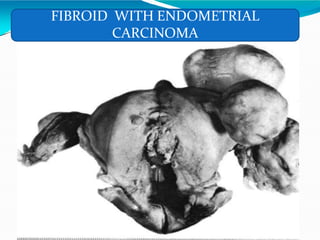
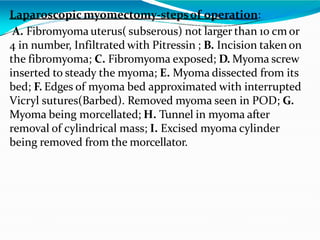
The document discusses uterine fibroids, which are benign tumors arising from the smooth muscle cells of the uterus. Key points include:
- Fibroids are the most common tumors found in the uterus, affecting 20-40% of women. Common symptoms include abnormal uterine bleeding, infertility, pain, and pressure effects.
- The exact cause is unknown but fibroids are influenced by genetic, hormonal, and growth factors. They are estrogen-dependent and usually regress after menopause.
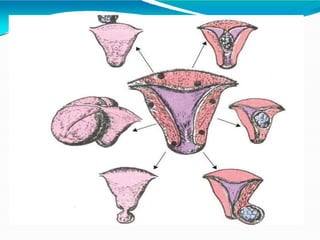
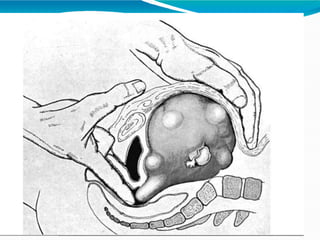
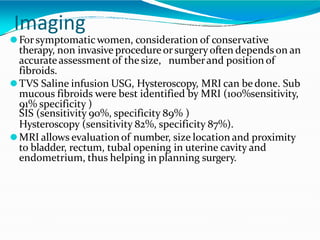
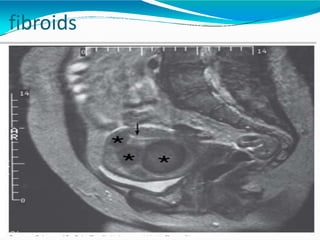
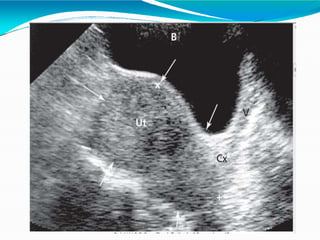
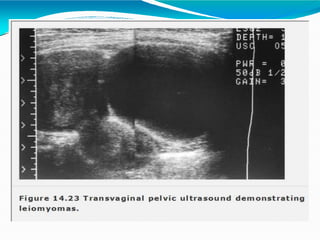
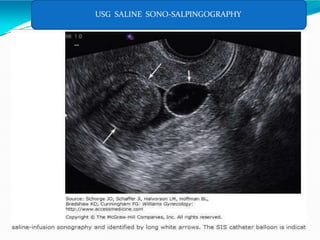
- Diagnosis involves physical exam, ultrasound, MRI or hysteroscopy to determine size, number and location of fibroids which helps guide treatment planning.
- Most fibroids grow slowly but can cause symptoms related to