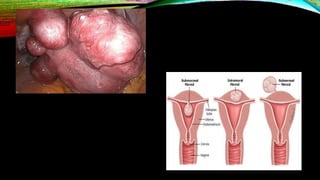
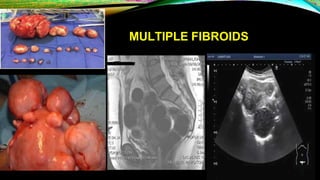
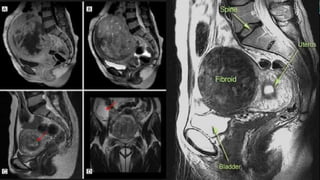
Uterine fibroids are benign muscle tumors that are the most common pelvic tumor in women. Symptoms include heavy bleeding, pelvic pressure, and reproductive issues. Evaluation involves physical exam, ultrasound, and sometimes MRI. Treatment options include medical management, minimally invasive procedures like uterine artery embolization, and surgical options like myomectomy or hysterectomy.