Downloaded 112 times

![Message learnt
• The bundles were not intended to be comprehensive
care; rather, they were developed to test a theory —
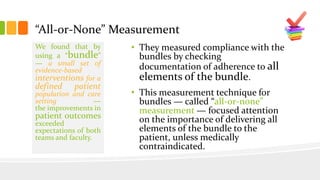
that is, when compliance is measured for a core set of
accepted elements of care for a clinical process, the
necessary teamwork and cooperation required will
result in high levels of sustained performance
[reliability] not observed when working to improve
individual elements.](https://image.slidesharecdn.com/477bf4e5-ee99-4abb-ab73-dbbb59322951-151206102931-lva1-app6891/85/Using-Care-Bundles-13-320.jpg)
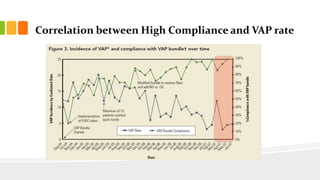
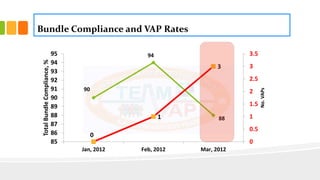



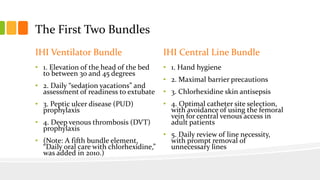
The document describes the development and use of care bundles over the past decade to improve health care quality. It discusses that care bundles were originally developed by the Institute for Healthcare Improvement (IHI) and Voluntary Hospital Association (VHA) in 2001 to improve critical care processes and outcomes. The first two bundles developed were the ventilator-associated pneumonia (VAP) bundle and central line-associated bloodstream infection (CLABSI) bundle. When compliance with the bundles was measured using an "all-or-none" approach, both VAP and CLABSI rates decreased significantly, demonstrating the effectiveness of the bundle approach. The document outlines guidelines for designing effective care bundles, including that they should have 3-5 evidence