WHY CARE BUNDLE?
•Care “bundles” are simple sets of evidence-based practices that,
when implemented collectively
, improve the reliability of their
delivery and improve patient outcomes.
• A number of specific bundles are available that can be
implemented at healthcare facilities in resource-limited settings.
• These packages of care contribute to infection prevention, reduce
unnecessary antibiotic prescribing, and may limit the
development of antibiotic resistance in healthcare facilities
3.
WHAT WILL BETHE OUTCOME?
• The implementation of care bundles can assist in enhancing compliance to evidence-
based quality process measures to improve patient care.
• Care bundles include a set of evidence-based measures.
• Bundles also help to create reliable and consistent care systems in hospital settings
since they are simple (three to five elements), clear
, and concise.
• In addition to creating safer patient care environments, the implementation of
bundles also promotes multi-disciplinary collaboration, since they should be
developed collaboratively and consensus obtained with strong clinician
engagement and endorsement.
4.
HOW IT CANBE SUCCESSFUL?
• Implemented collectively with complete consistency. (“all or none” approach).
• Care bundle requires local setting; appropriately followed; rooted in the patient
care culture and; recorded and evaluated to ensure compliance by all members
of the healthcare team involved.
• Each bundle element for every patient, always.
5.
• Bundled interventionsare an effective way to implement
change and improve the “culture” of patient safety by
promoting teamwork, measuring compliance and
providing feedback and accountability to frontline
teams and hospital leadership to improve care.
6.
IMPLEMENTATION STRATEGIES:
• Amulti-disciplinary approach, coupled with an institution-
wide multi-modal strategy including: will-building, awareness,
training, education, measurement, and feedback are
required to optimally promote and sustain the
implementation of care bundles in hospital settings.
7.
• Healthcare teammembers are clear on the elements of each bundle, the
actions required and, how compliance is measured and tracked for feedback.
• Bundle require particular supplies or products, these should be
appropriately procured prior to bundle roll-out and implementation.
• The elements of a bundle are measured in an “all or nothing” manner to
simplify assessment of compliance for feedback to providers and to emphasize
the completion of every component.
• A bundle compliance percentage goal should be set for the healthcare team
to work toward achieving (95% bundle compliance is the recommended best
practice)
CENTRAL LINE-ASSOCIATED BLOODSTREAM
INFECTIONS(CLABSI).
• Bundles for the prevention of central line-associated bloodstream infections
(CLABSI) Central lines are used commonly in
• intensive care units (ICUs)
• Non ICU populations such as dialysis units, intraoperatively, and oncology patients.
• Most hospital-acquired bloodstream infections are associated with a central line
(including peripherally-inserted central catheters, PICCs), and CLABSIs are
responsible for excess mortality and morbidity, prolonged hospital stays, and
increased costs.
• CLABSI incidence is higher in low-income countries.
• Implementation of central line insertion and maintenance bundles reduces the
incidence of CLABSI in ICUs and nonICU settings including in low-income countries.
12.
INSERTION BUNDLE: -
•CLABSI prevention bundles include the following components.
• Maximal sterile barrier precautions (surgical mask, sterile gloves, cap, sterile gown, and large sterile
drape).
• Skin cleaning with alcohol-based chlorhexidine (rather than iodine).
• - Avoidance of the femoral vein for central venous access in adult patients; use of subclavian rather than
jugular veins.
• - Dedicated staff for central line insertion, and competency training/assessment Standardized insertion
packs.
• - Availability of insertion guidelines (including indications for central line use) and use of checklists with
trained
observers.
• - Use of ultrasound guidance for insertion of internal jugular lines.
15.
MAINTENANCE BUNDLE: -
•. Daily review of central line necessity.
• - Prompt removal of unnecessary lines.
• - Disinfection prior to manipulation of the line.
• - Daily chlorhexidine washes (in ICU, patients > 2 months).
• - Disinfect catheter hubs, ports, connectors, etc., before using the catheter.
• - Change dressings and disinfect site with alcohol-based chlorhexidine every 5-7 days (change
earlier if soiled).
• - Replace administration sets within 96 hours (immediately if used for blood products or
lipids).
• - Ensure appropriate nurse-to-patient ratio in ICU
17.
• These activitiesneed to be integrated in a multi-modal approach
including hand hygiene, clinician and nurse education, and
performance of surveillance and feedback of CLABSI rates.
18.
BUNDLE FOR THEPREVENTION OF CATHETER-
ASSOCIATED URINARY TRACT INFECTIONS (CAUTI):
• CAUTI is defined as a urinary tract infection (significant bacteriuria plus
symptoms and/or signs attributable to the urinary tract with no other
identifiable source) in a patient with current urinary tract catheterization or
who has been catheterized in the past 48 hours.
• It is the most common healthcare associated infection worldwide, resulting
in increased costs, hospital stays, and substantial morbidity.
• The majority of cases are considered to be avoidable with the
implementation of infection prevention bundles of care.
19.
• There area number of strategies with varying levels of evidence to prevent
CAUTI before and after placement of urinary catheters.
• These generally include appropriate use,
• aseptic insertion and maintenance,
• early removal, and hand hygiene.
• Recently, a large study in the United States demonstrated that a simple
intervention comprising three components reduced catheter use and CAUTI
rates in non-ICU acute care settings:
21.
SIMPLE PREVENTION CANREDUCE CAUTI IN
NON ICU
• Avoiding the use of urinary catheters by considering alternative methods for urine collection.
• - Methods include: condom catheters, intermittent catheterization, use of nappies.
• Using an aseptic technique for insertion and proper maintenance after insertion. - Following
evidence-based guidelines and implementing catheter insertion policies at the institution.
• . Daily assessment of the presence and need for indwelling urinary catheters.
• - Indications for urinary catheterization include:
• - Urinary retention (mechanical obstruction or neuropathic). - Need to closely monitor urine
output in unstable patients.
• - To assist perineal wound care
23.
• The bundleabove is implementable in resource-poor settings, and
should be accompanied by a multimodal approach of hand hygiene,
healthcare worker education, and feedback of catheter use and
CAUTI rates.
25.
BUNDLE FOR THEPREVENTION OF VENTILATOR
ASSOCIATED PNEUMONIA (VAP)
• VAP
, defined as a new pneumonia occurring > 48 hours after endotracheal intubation, is a
common and serious hospital-acquired infection.
• It occurs in up to 20% of patients receiving mechanical ventilation, and is associated with
increased antibiotic use, length of hospitalization, and healthcare costs.
• The mortality associated with VAP ranges from 20% to 50%, and the attributable
mortality is estimated at 13%.20 It has been estimated that over half the cases of VAP
may be preventable with evidence-based strategies, with an impact on mortality.
26.
BUNDLE OF VENTILATORCARE PROCESSES THAT
REDUCE VAP RATES:-
• Elevate the head of the bed to between 30 and 45 degrees.
• • Daily “sedation interruption” and daily assessment of readiness to extubate.
• • Daily oral care with chlorhexidine.
• • Prophylaxis for peptic ulcer disease.
• • Prophylaxis for deep venous thrombosis
28.
• These interventionsshould be implemented together with standard precautions
(hand hygiene and use of gloves when handling respiratory secretions) as well as
adequate disinfection and maintenance of equipment and devices.
• Other components of the VAP bundle may include:
• • Utilization of endotracheal tubes with subglottic secretion drainage (only for
patients
ventilated for longer than 24 hours)
• • Initiation of safe enteral nutrition within 24-48 hours of ICU admission
29.
BUNDLE FOR THEPREVENTION OF SURGICAL
SITE INFECTION (SSI)
• SSIs are infections of the incision or organ or space that occur after
surgery.
• SSIs complicate ~1.9% of surgical procedures in the United States, and
result in excessive healthcare costs.
• In contrast, infection is the most common postoperative
complication in African countries, occurring in 10% of procedures; it
is associated with a 9.7% case fatality rate.
• It has been estimated that approximately half of SSIs are
preventable.
30.
BUNDLE OF CARETO PREVENT
SSI:
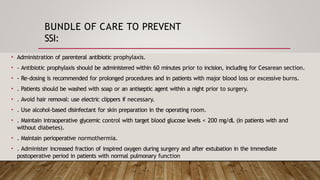
• Administration of parenteral antibiotic prophylaxis.
• - Antibiotic prophylaxis should be administered within 60 minutes prior to incision, including for Cesarean section.
• - Re-dosing is recommended for prolonged procedures and in patients with major blood loss or excessive burns.
• . Patients should be washed with soap or an antiseptic agent within a night prior to surgery.
• . Avoid hair removal: use electric clippers if necessary.
• . Use alcohol-based disinfectant for skin preparation in the operating room.
• . Maintain intraoperative glycemic control with target blood glucose levels < 200 mg/dL (in patients with and
without diabetes).
• . Maintain perioperative normothermia.
• . Administer increased fraction of inspired oxygen during surgery and after extubation in the immediate
postoperative period in patients with normal pulmonary function
31.
• The interventionsabove should be implemented with a
multimodal package of infection prevention including hand
hygiene, sterilization of surgical equipment, the use of
appropriate surgical attire, and staff education and
feedback
32.
SUGGESTED PRACTICE INUNDER-RESOURCED
SETTINGS:
• • Implementation of infection prevention care bundles, such as the CLABSI bundle, have
been shown to be as effective in restricted resource, low- and middle-income countries
when compared to their higher-income counterparts.
• • The most effective programs include those with robust leadership, stringent protocols,
participation of all members of the available healthcare team, reliable measurement of
compliance, subsequent feedback of results, and the enablement of nursing staff to stop
practice if the required protocols are not appropriately followed by other team
members.
REFERENCE:
• GUIDE TOINFECTION CONTROL IN THE HOSPITAL CHAPTER 16: Bundles
in
Infection Prevention and Safety
Editor's Notes
#2 What is a Care Bundle and Why Does it Matter?
Care bundles are like checklists of simple, science-backed actions that, when used together, help make patient care safer, more reliable, and more effective — especially in hospitals with fewer resources.
A care bundle is a small, focused group of proven medical practices or steps that are meant to be done together. Each step is based on solid evidence, and when all steps in the bundle are done as a group — not just one or two — they lead to better results for patients.
Why Use Care Bundles in Healthcare Settings, Especially in Low-Resource Areas?
In places where there are limited resources (like fewer staff, supplies, or money), these bundles help healthcare workers stay organized and consistent in providing good care.
Specific care bundles are already developed and ready to be used in these settings.
They help with:
Preventing infections
Reducing the use of unnecessary antibiotics
Slowing down antibiotic resistance — which is when bacteria stop responding to antibiotics, making infections harder to treat.
#3 Why Implement Care Bundles?
Implementing care bundles helps improve patient care in several important ways:
1. Improves Compliance with Best Practices
Care bundles are built on evidence-based quality measures — meaning, these are steps that research has shown actually work. Using them helps hospitals stick to the best medical practices more reliably.
2. They Are Simple and Easy to Follow
A bundle usually includes just three to five key steps.
This makes them clear, concise, and easy to remember, even in busy hospital environments.
Because of their simplicity, they're more likely to be used correctly and consistently.
3. Creates Reliable and Consistent Care
Bundles help standardize care, so no matter who the healthcare provider is, the patient receives the same high-quality care every time. This reduces errors and improves safety.
4. Encourages Teamwork and Collaboration
Bundles aren’t created in isolation. They should be developed and agreed upon by the whole care team — doctors, nurses, and other healthcare workers.
This encourages multi-disciplinary teamwork and ensures everyone is on the same page.
When everyone contributes and agrees, there's stronger buy-in and engagement, making implementation more successful.
#4 ✅ How to Successfully Implement a Care Bundle
To make a care bundle truly effective, it’s not just about having the right steps — it’s about how they’re applied. Here's what it takes:
1. “All or None” Approach
A care bundle only works if every element is completed for every patient, every time.
If even one step is missed, it’s considered non-compliant.
This approach raises the standard of care and prevents cutting corners.
Think of it like baking a cake — skipping just one ingredient could ruin the whole thing.
2. Tailored to the Local Setting
The bundle must fit the specific environment of the hospital or clinic (e.g., available resources, staffing, patient population).
You can’t just copy and paste a bundle from somewhere else — it needs to be adapted to what’s realistic and relevant locally.
3. Part of the Care Culture
Staff need to believe in the value of the bundle — it should become part of the hospital’s routine way of doing things.
This means ongoing training, support, and leadership involvement are key to build it into the daily flow of care.
#5 1. Promote Teamwork
Bundles are designed to be followed by all members of the care team.
Because everyone plays a role, bundles naturally encourage collaboration, communication, and shared responsibility.
This improves not just the quality of care, but the team dynamic, too.
2. Create a Culture of Safety
When bundles are used consistently, they help build a standardized way of working that prioritizes safety and best practices.
This consistency helps staff feel more confident and accountable, which leads to a more safety-focused environment.
3. Measure Compliance
You can’t improve what you don’t measure. Bundles provide clear, trackable steps.
Hospitals can monitor whether each element is being done, for every patient.
This allows for real-time performance data, helping teams see how well they’re doing.
4. Provide Feedback and Accountability
Teams receive feedback on their performance, which is key for improvement.
If something isn’t working, the team can see the data and adjust quickly.
This creates a loop of learning, accountability, and continuous improvement.
5. Engage Leadership and Frontline Teams
Successful bundle use involves both the frontline staff (who deliver care) and hospital leaders (who support resources and policy).
When both levels are engaged, the chances of sustainable change are much higher.
#6 🏥 How to Successfully Promote and Sustain Care Bundle Implementation
To truly make care bundles effective and long-lasting, hospitals need more than just good intentions — they need a multi-disciplinary and multi-modal strategy.
Here’s what that includes:
🔁 1. Multi-Disciplinary Approach
Involves all key healthcare professionals — doctors, nurses, pharmacists, infection control teams, etc.
Promotes collaboration across departments and levels of care.
Ensures that every perspective is considered, increasing buy-in and teamwork.
🛠️ 2. Multi-Modal Strategy: What’s Needed?
A mix of several key elements is required:
✔️ Will-Building:
Create motivation and commitment to change — leadership must support and champion the bundle.
✔️ Awareness:
Everyone must understand why the care bundle matters and how it improves patient outcomes.
✔️ Training & Education:
Staff need to be properly trained on how to implement each part of the bundle — consistently and correctly.
✔️ Measurement:
Track performance — how often are all bundle steps completed as intended?
✔️ Feedback:
Share results with the team. Celebrate successes, identify gaps, and continuously improve.
🔑 Why This Matters
Together, these strategies help:
Build a culture of accountability
Promote continuous learning
Ensure the care bundle becomes a standard part of care, not just a checklist
#7 1. Clarity for Healthcare Teams
All team members must be fully aware of:
The specific elements of each care bundle
The required actions for each element
How compliance will be measured and tracked
This ensures consistency and avoids confusion during implementation.
2. Supply Preparedness
If the bundle requires specific products or supplies (e.g., sterile equipment, hand hygiene materials), these must be:
Identified early
Procured and available before the bundle is rolled out
This prevents delays and gaps in implementation.
3. “All or Nothing” Measurement
Compliance is assessed only when every element of the bundle is completed.
This method:
Simplifies tracking
Encourages full adherence rather than partial compliance
Reinforces that every step matters
4. Set a Clear Compliance Goal
A target compliance rate should be set for the healthcare team.
Best practice goal:
✅ 95% bundle compliance
Setting a clear, ambitious benchmark:
Creates a shared goal to work toward
Provides a basis for performance feedback
Drives improvement through team accountability
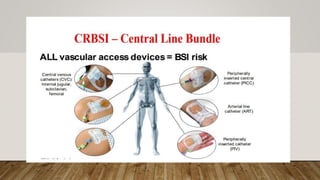
#9 his image illustrates the concept of CRBSI – Central Line Bundle, highlighting that all vascular access devices carry a risk of bloodstream infection (BSI), not just central lines. The image maps out various vascular access points on a human figure and emphasizes the need for strict adherence to infection prevention protocols.
Explanation in Light of Care Bundles:
A care bundle is a structured way of improving care processes and outcomes by ensuring consistent application of evidence-based practices. In the context of Catheter-Related Bloodstream Infections (CRBSIs), the Central Line Bundle refers to a set of best practices to reduce the risk of infection associated with central venous catheters (CVCs) and other vascular access devices.
Key Components of a Central Line Bundle:
Hand Hygiene
Before catheter insertion or manipulation, proper handwashing or use of alcohol-based hand rubs is critical to reduce microbial transmission.
Maximal Barrier Precautions
During insertion of central lines (e.g., CVC, PICC), full barrier precautions (mask, cap, sterile gown, sterile gloves, large sterile drape) are essential.
Chlorhexidine Skin Antisepsis
Proper antisepsis of the insertion site using chlorhexidine reduces skin flora that can cause infection.
Optimal Catheter Site Selection
Avoiding sites like the femoral vein when possible, due to higher infection risks. Prefer subclavian or internal jugular.
Daily Review of Line Necessity
Remove catheters as soon as they are no longer needed to reduce infection risk.
Vascular Access Devices Highlighted in the Image:
CVCs (Central Venous Catheters) – Internal jugular, subclavian, femoral
PICC (Peripherally Inserted Central Catheter)
ART (Arterial Line Catheter)
PIV (Peripheral Intravenous Catheter)
While central line bundles are primarily designed for CVCs, the bundle approach can be adapted for all catheter types because all are potential sources of infection.
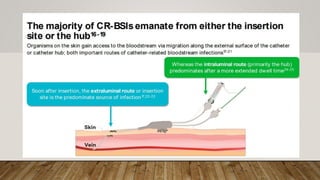
#10 Two Primary Routes of CRBSI:
Extraluminal route: Occurs via the insertion site, where skin flora migrate along the external surface of the catheter.
Intraluminal route: Infection occurs through the hub or connector, migrating internally along the catheter lumen.
Time-Specific Infection Risk:
Early infections (soon after insertion) → Extraluminal route predominates.
Later infections (prolonged catheter use) → Intraluminal route predominates.
🩺 Clinical Relevance for Care Bundles:
In the early stage (focus on extraluminal route):
Aseptic insertion technique is crucial.
Use of chlorhexidine for skin antisepsis.
Maximal sterile barrier precautions (gloves, gown, mask, drape).
Choose optimal insertion site (avoid femoral when possible).
In the later stage (focus on intraluminal route):
Disinfection of catheter hubs before every access (e.g., alcohol caps or scrubs).
Closed system maintenance to reduce entry points for microbes.
Avoid frequent manipulation of the catheter line.
#11 Overview:
Central lines are widely used in:
Intensive Care Units (ICUs)
Non-ICU settings such as dialysis units, operating rooms, and among oncology patients.
Most hospital-acquired bloodstream infections are associated with central lines, including Peripherally-Inserted Central Catheters (PICCs).
CLABSIs contribute to:
Increased mortality and morbidity
Prolonged hospital stays
Higher healthcare costs
Global Perspective:
CLABSI incidence is higher in low-income countries.
Resource limitations and lack of standardized protocols contribute to this increased burden.
Impact of Care Bundles:
The implementation of central line insertion and maintenance bundles has been shown to:
Significantly reduce the incidence of CLABSI
Improve outcomes both in ICU and non-ICU settings
Be effective even in low-income countries
#12 Core Components:
🔴 Maximal Sterile Barrier Precautions:
Surgical mask
Sterile gloves
Sterile gown
Cap
Large sterile drape
🔴 Skin Antisepsis:
Use alcohol-based chlorhexidine for skin cleaning before insertion (preferred over iodine).
🔴 Site Selection:
Avoid the femoral vein for central access in adults. (The femoral area is close to the groin, which has higher bacterial colonization. Sweat, moisture, and proximity to the perineum create a warm, moist environment ideal for bacterial growth.)
Prefer subclavian vein over the internal jugular vein for lower infection risk.
🔴 Trained Personnel:
Dedicated staff responsible for central line insertions.
Regular competency training and skills assessment for all staff involved.
🔴 Standardized Insertion Packs:
Use prepared, standardized kits to ensure all necessary sterile items are available.
🔴 Use of Checklists and Guidelines:
Central line insertion checklists used during every procedure.
Trained observers monitor compliance in real-time.
Clear insertion guidelines including appropriate indications for line placement.
🔴 Ultrasound Guidance:
Use ultrasound for safer and more accurate insertion of internal jugular vein catheters.
#15 Key Practices:
🔵 Daily Review of Central Line Necessity:
Assess every day if the line is still needed.
Remove the central line promptly once it is no longer necessary.
🔵 Disinfection Before Manipulation:
Always disinfect catheter hubs, ports, and connectors before accessing or using the line.
Use alcohol-based solutions or chlorhexidine wipes.
🔵 Daily Chlorhexidine Bathing:
Perform daily chlorhexidine washes for ICU patients older than 2 months.
Reduces skin colonization and infection risk.
🔵 Proper Site and Dressing Care:
Change dressings every 5–7 days (or sooner if soiled, loose, or damp).
Disinfect the insertion site with alcohol-based chlorhexidine at every dressing change.
🔵 Timely Replacement of Administration Sets:
Replace IV tubing and administration sets within 96 hours routinely.
Replace immediately if the set was used for blood products, lipids, or parenteral nutrition.
🔵 Safe Staffing Levels:
Maintain appropriate nurse-to-patient ratios in ICU to allow time for proper line care and monitoring.
#18 Definition of CAUTI:
A catheter-associated urinary tract infection (CAUTI) occurs when there is significant bacteriuria plus urinary symptoms/signs without another identifiable infection source.
It happens in patients with a current urinary catheter or within 48 hours of catheter removal.
Impact:
Most common healthcare-associated infection globally.
Leads to increased healthcare costs, prolonged hospital stays, and substantial patient morbidity.
Majority of CAUTIs are preventable with appropriate infection prevention bundles.
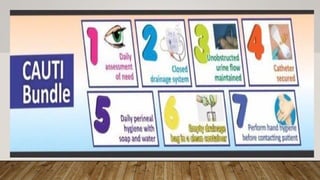
Key Elements of a CAUTI Prevention Bundle:
🔵 Avoid Unnecessary Catheterization:
Insert catheters only when clinically indicated (e.g., urinary retention, accurate urine output monitoring in critically ill patients).
🔵 Aseptic Insertion Technique:
Use sterile equipment and maintain aseptic technique during catheter insertion.
Trained staff should insert catheters following strict protocols.
🔵 Maintain Closed Drainage System:
Ensure the catheter and drainage system remain closed and intact to prevent bacterial entry.
🔵 Daily Review of Catheter Need:
Assess catheter necessity daily and remove the catheter as soon as possible when no longer needed.
🔵 Secure Catheter Properly:
Anchor the catheter to prevent movement and urethral trauma, reducing infection risk.
🔵 Maintain Unobstructed Urine Flow:
Keep the drainage bag below bladder level and prevent kinking or obstruction of the catheter tubing.
🔵 Hand Hygiene:
Perform hand hygiene before and after manipulating the catheter or drainage system.
🔵 Routine Catheter Care:
Perform regular perineal hygiene.
Do not routinely change catheters or drainage bags unless clinically indicated.
#19 Key Strategies:
🔹 Appropriate Use:
Only insert urinary catheters when medically necessary.
Avoid catheterization for convenience or routine urine output monitoring in non-critically ill patients.
🔹 Aseptic Insertion and Maintenance:
Use sterile technique during insertion.
Maintain a closed, sterile drainage system post-insertion to minimize contamination.
🔹 Early Removal:
Daily reassessment of the need for the catheter.
Prompt removal as soon as it's no longer essential for patient care.
🔹 Hand Hygiene:
Strict hand washing before and after any catheter manipulation to prevent introducing organisms.
Recent Evidence - Simple Three-Part Intervention:
A large U.S. study found that a simple bundle intervention could significantly reduce both catheter use and CAUTI rates in non-ICU acute care settings.
The three components were:
Nurse-Driven Protocols for Catheter Removal:
Nurses empowered to assess catheter need daily and remove catheters without waiting for physician orders if clinical criteria were met.
Standardized Catheter Insertion Checklists:
Use of checklists to ensure aseptic technique and appropriate indications at the time of catheter insertion.
Feedback on Catheter Use and CAUTI Rates:
Monitoring catheter utilization rates and regularly sharing data with frontline staff to encourage compliance and improve performance.
#21 ✅ Key Prevention Strategies:
🔹 Avoid Unnecessary Catheterization:
Always consider alternatives to indwelling urinary catheters:
Condom catheters (for male patients)
Intermittent catheterization
Use of absorbent pads or nappies when appropriate
🔹 Use Aseptic Insertion Technique:
Ensure strict aseptic technique during insertion.
Follow evidence-based guidelines and institutional protocols.
Provide training and competency checks for staff.
🔹 Proper Catheter Maintenance:
Keep the system closed and unobstructed.
Perform daily perineal hygiene and disinfect hands before/after any contact.
🔹 Daily Assessment of Catheter Need:
Review catheter use every day.
Promptly remove when no longer indicated.
📌 Indications for Urinary Catheterization:
Urinary retention
Due to mechanical obstruction or neurological conditions
Accurate urine output monitoring
In critically ill or unstable patients
Facilitation of wound healing
In patients with extensive perineal wounds or skin breakdown
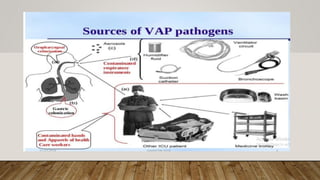
#24 This image illustrates the various sources of pathogens responsible for ventilator-associated pneumonia (VAP) in intensive care unit (ICU) patients.
Key Sources of VAP Pathogens:
Oropharyngeal colonization: Microorganisms from the mouth and throat can enter the lower respiratory tract, especially in intubated patients.
Gastric colonization: Bacteria from the stomach can ascend into the lungs, particularly when the normal protective mechanisms are bypassed.
Contaminated respiratory instruments: Medical devices such as ventilator circuits, humidifier fluids, suction catheters, and bronchoscopes can harbor and transmit pathogens if not properly sterilized.
Aerosols: Pathogens can be transmitted through airborne particles.
Contaminated hands and apparel of healthcare workers: Improper hand hygiene and contaminated clothing of healthcare staff can transfer pathogens to patients.
Other ICU patients and surfaces: Pathogens can spread via contact with other patients, medicine trolleys, wash basins, and other surfaces in the ICU environment.
#25 🦠 What is VAP?
Ventilator-Associated Pneumonia (VAP) is a new pneumonia that develops >48 hours after endotracheal intubation.
Affects up to 20% of patients on mechanical ventilation.
⚠️ Why It Matters:
Leads to increased use of antibiotics
Causes longer hospital stays and higher healthcare costs
Mortality rate ranges from 20% to 50%
Attributable mortality is estimated at 13%
Over half of VAP cases may be preventable through evidence-based practices
#26 ✅ Key Strategies in the VAP Prevention Bundle:
Elevate the Head of the Bed:
Keep the head of the bed at 30–45° to prevent aspiration.
Daily Sedation Interruption and Assessment of Readiness to Extubate:
Conduct "sedation vacations" and check if the patient can be weaned off the ventilator.
Oral Care with Chlorhexidine:
Provide regular oral care using chlorhexidine solution (0.12%–0.2%).
Peptic Ulcer and Deep Vein Thrombosis (DVT) Prophylaxis:
Prevent secondary complications, especially in long-term ventilated patients.
Subglottic Secretion Drainage:
Use endotracheal tubes with subglottic suction ports to reduce pooled secretions.
Hand Hygiene and Infection Control:
Maintain strict hand hygiene before and after any airway manipulation.
Avoid Unnecessary Ventilation:
Minimize duration of mechanical ventilation; extubate early when safe.
#27 VAP Bundle
The VAP bundle consists of four main interventions:
Head of bed elevation (30–45 degrees): Elevating the head of the bed reduces the risk of aspiration, which is a major cause of VAP.
Oral care with chlorhexidine: Regular oral hygiene with an antiseptic (chlorhexidine) decreases bacterial colonization in the mouth and oropharynx, reducing the risk of infection.
Sedation vacation: Periodically stopping sedation allows assessment of the patient's readiness to breathe independently, which can reduce the duration of mechanical ventilation and associated risks.
Weaning trials: Daily trials to assess the patient's ability to breathe without the ventilator help minimize the time on mechanical ventilation, further lowering infection risk.
VAE Bundle
The VAE bundle includes all the VAP bundle components plus additional measures:
Head of bed elevation (30–45 degrees)
Oral care with chlorhexidine
Sedation vacation
Weaning trials
DVT & PUD prophylaxis: Additional steps are included to prevent deep vein thrombosis (DVT) and peptic ulcer disease (PUD), which are common complications in critically ill, immobilized patients.
#28 1. Standard Precautions
Hand Hygiene: Ensure rigorous hand hygiene, following the 5 Moments of Hand Hygiene. Perform hand hygiene before and after patient contact, after touching the environment or medical equipment, and after contact with respiratory secretions.
Use of Gloves: Always wear gloves when handling respiratory secretions or when touching areas that might be contaminated, like ventilator tubing or the patient's mouth and airway.
2. Adequate Disinfection and Maintenance of Equipment
Ventilator Circuit and Accessories: Clean and disinfect ventilator circuits, suction catheters, and respiratory devices regularly. Ensure disposable items are discarded properly.
Regular Monitoring of Equipment: Ensure that ventilator equipment is well-maintained, with routine checks for malfunction, condensation in the tubing, and proper functionality.
3. Key Components of the VAP Bundle
Utilization of Endotracheal Tubes with Subglottic Secretion Drainage
Indication: This is recommended for patients who are expected to be ventilated for more than 24 hours. The goal is to prevent secretion accumulation in the subglottic area, which can serve as a breeding ground for pathogens that lead to VAP.
Implementation: Use endotracheal tubes with a subglottic secretion drainage port to facilitate the continuous or intermittent drainage of secretions above the cuff, thereby reducing the risk of aspiration and VAP.
Initiation of Safe Enteral Nutrition
Timing: Enteral nutrition should be initiated within 24-48 hours of ICU admission, even if the patient is intubated.
Rationale: Early enteral feeding has been shown to reduce the risk of infection, improve outcomes, and prevent complications like gastric distension, which can increase the risk of aspiration.
Implementation: Use a nasogastric (NG) or nasoduodenal tube to provide enteral nutrition. Elevate the head of the bed to at least 30-45 degrees to reduce the risk of aspiration during feeding.
#29 The Bundle for the Prevention of Surgical Site Infection (SSI) is designed to reduce the risk of infections following surgery. Implementing a bundle approach involves a series of evidence-based interventions that are performed consistently to enhance patient outcomes and minimize the risk of SSIs. Given the significant impact of SSIs on both healthcare costs and patient health outcomes, it's essential that these interventions are applied systematically.
SSIs are a significant complication in surgeries, with about 1.9% of procedures in the United States resulting in infection, leading to high healthcare costs. In African countries, the incidence is notably higher, with 10% of surgeries affected by infection and a 9.7% case fatality rate. Studies suggest that approximately 50% of SSIs are preventable through the implementation of preventive measures, often bundled together for more effective risk reduction.
#30 The Bundle of Care to Prevent Surgical Site Infection (SSI) consists of several key practices aimed at reducing the risk of infection after surgery:
Parenteral Antibiotic Prophylaxis: Administer antibiotics within 60 minutes before surgery, including Cesarean sections. For prolonged surgeries or patients with significant blood loss or burns, re-dosing may be required.
Preoperative Hygiene: Patients should be washed with soap or an antiseptic agent the night before surgery to reduce microbial load.
Hair Removal: Avoid shaving the surgical area. If hair removal is necessary, use electric clippers to minimize skin trauma.
Skin Preparation: Use alcohol-based disinfectants for skin preparation in the operating room to reduce bacteria at the surgical site.
Glycemic Control: Maintain intraoperative blood glucose levels below 200 mg/dL, regardless of whether the patient has diabetes, to reduce infection risk.
Normothermia: Ensure that the patient remains normothermic (normal body temperature) during surgery to prevent complications related to hypothermia.
Oxygenation: Administer a higher fraction of inspired oxygen during surgery and in the immediate postoperative period to patients with normal pulmonary function, which helps in reducing infection risk and improving tissue oxygenation.
#32 In under-resourced settings, the implementation of infection prevention care bundles, such as the Central Line-Associated Bloodstream Infection (CLABSI) bundle, has proven to be as effective as in higher-income settings. This is especially true when resources are limited, demonstrating that simple yet consistent infection control measures can significantly reduce infections.
The most effective infection prevention programs in low- and middle-income countries include:
Robust Leadership: Strong leadership is critical in driving the success of infection prevention initiatives, ensuring commitment and direction.
Stringent Protocols: Clear, well-established protocols need to be followed to maintain standard practices across all levels of care.
Team Participation: Engaging all healthcare team members in infection prevention practices ensures collaboration and adherence to protocols.
Reliable Measurement and Compliance Tracking: Monitoring compliance with the protocols and measuring outcomes consistently is essential for identifying gaps and improving practices.
Feedback Systems: Providing timely feedback based on measurement results helps maintain accountability and encourages continuous improvement.
Empowering Nursing Staff: Nursing staff should be empowered to halt procedures if protocols are not being followed, ensuring patient safety and adherence to infection prevention standards.
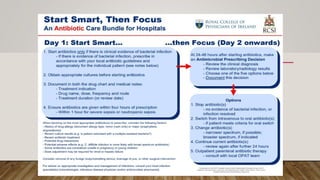
#34 This image outlines an antibiotic care bundle for hospitals, emphasizing a structured approach to antibiotic use to optimize treatment and minimize resistance. The bundle is divided into two main phases: "Start Smart" on Day 1 and "Then Focus" from Day 2 onwards.
Day 1: Start Smart
This phase focuses on the appropriate initiation of antibiotics.
Start antibiotics only if there is clinical evidence of bacterial infection: Antibiotics should only be started if there is a clear indication of a bacterial infection, following local antibiotic guidelines.
Obtain appropriate cultures before starting antibiotics: Taking cultures before starting antibiotics helps identify the specific bacteria causing the infection, which can guide future treatment decisions.
Document in both the drug chart and medical notes: Document the indication for antibiotic use, the drug name, dose, frequency, route, and the treatment duration or review date.
Ensure antibiotics are given within four hours of prescription Antibiotics should be administered promptly, ideally within one hour for severe sepsis or neutropenic sepsis.
Then Focus (Day 2 Onwards)
This phase involves reassessing the antibiotic regimen based on clinical and laboratory findings.
Make an Antimicrobial Prescribing Decision: At 24-48 hours after starting antibiotics, make an antimicrobial prescribing decision, including:
Review the clinical diagnosis
Review laboratory/radiology results
Choose one of the five options below
Document this decision
Options:
Stop antibiotic(s): If there is no evidence of bacterial infection or if the infection is resolved.
Switch from intravenous to oral antibiotic(s): If the patient meets criteria for oral switch.
Change antibiotic(s): Adjust to a narrower or broader spectrum antibiotic, if indicated.
Continue current antibiotic(s): Reassess again after a further 24 hours.
Outpatient parenteral antibiotic therapy: Consult with the OPAT team.
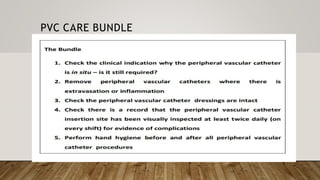
#35 A Peripheral Venous Catheter (PVC) care bundle includes the following steps:
Check the clinical indication: Determine if the peripheral vascular catheter is still necessary.
Remove unnecessary catheters: Remove PVCs where there is extravasation or inflammation.
Check the dressing: Ensure the peripheral vascular catheter dressings are intact.
Monitor insertion site: Confirm that the peripheral vascular catheter insertion site has been visually inspected at least twice daily (on every shift) for evidence of complications.
Perform hand hygiene: Always practice proper hand hygiene before and after all peripheral vascular catheter procedures.