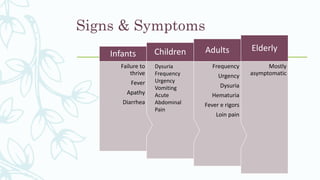
Urinary tract infections (UTIs) are caused by the presence of microorganisms in the urinary tract. UTIs can be uncomplicated or complicated depending on whether there are underlying medical issues. Common symptoms include burning during urination, frequent urination, and abdominal pain. Diagnosis involves urine testing and culture. Treatment depends on whether the infection is uncomplicated or complicated but generally involves antibiotic therapy for 3-14 days depending on severity. Single dose antibiotics are often used for uncomplicated infections while longer courses are needed for complicated or recurrent UTIs.


















































![Multiple gestation [autosaved].pptx 1](https://cdn.slidesharecdn.com/ss_thumbnails/multiplegestationautosaved-191005181123-thumbnail.jpg?width=640&height=640&fit=bounds)

























