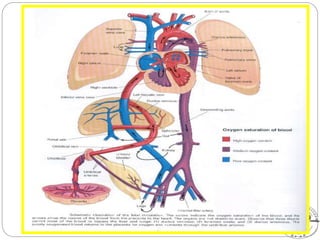
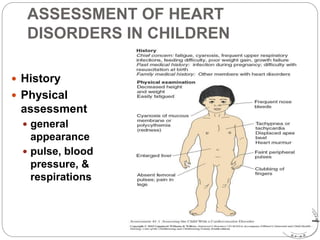
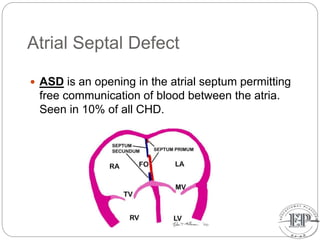
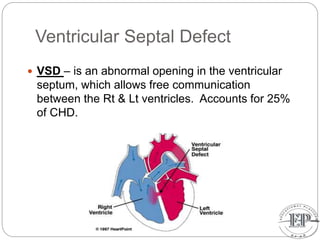
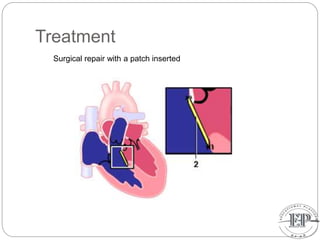
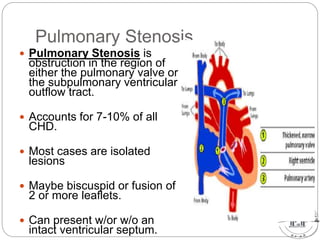
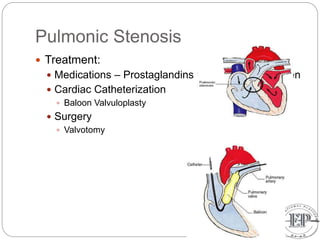
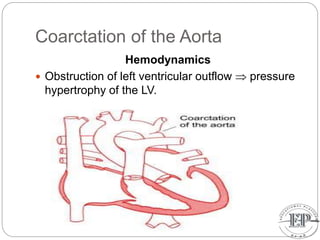
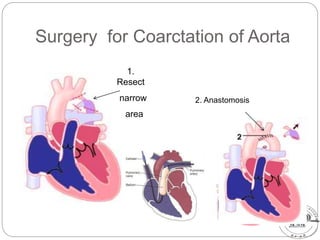
This document discusses fetal circulation and several congenital heart defects that can occur, including their pathophysiology, clinical presentation, and treatment. It begins by describing the normal fetal circulation, where oxygenated blood from the placenta travels through the umbilical vein, ductus venosus, and foramen ovale to supply the fetus. It then covers several defects: atrial septal defect, ventricular septal defect, patent ductus arteriosus, pulmonary stenosis, aortic stenosis, and coarctation of the aorta. For each, it provides an overview of how blood flow is disrupted, typical signs and symptoms, and treatment approaches like surgery, catheterization, or medication management.

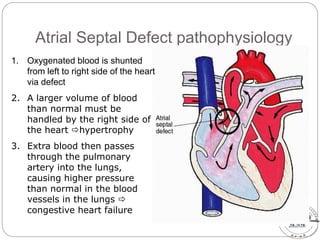
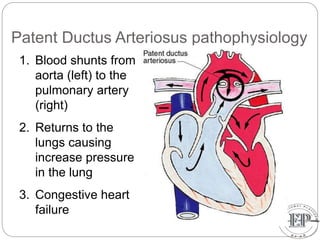
















![UNIT_9_FETAL_CIRCULLATION_and_malformation_of_heart[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/unit9fetalcircullationandmalformationofheart1-250618102701-ee5d1ff8-thumbnail.jpg?width=640&height=640&fit=bounds)































