Download to read offline






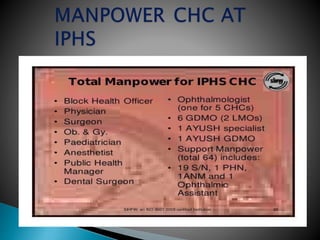
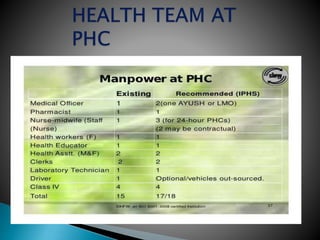
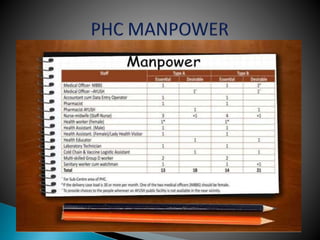
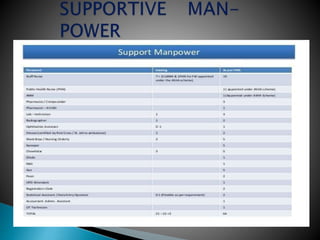
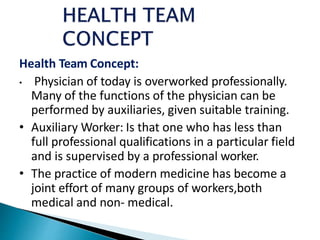
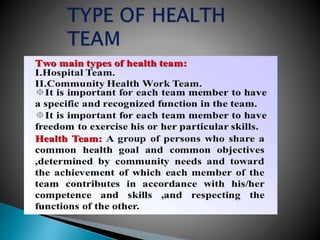
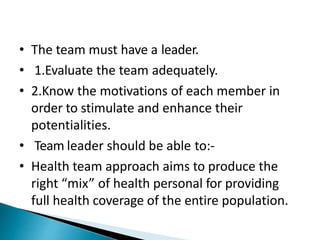



The document discusses the concept of a health team and its composition and functions. It describes the roles of various community health workers that make up the health team, including the district public health nursing officer, block health nurse, public health nurse, lady health visitors, and health workers. The health team aims to provide full health coverage to the population through a mix of health professionals working together under leadership. Each member has specific responsibilities for activities like supervising other health workers, conducting home visits, maintaining records and supplies, providing antenatal care, immunizations, and health education.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
