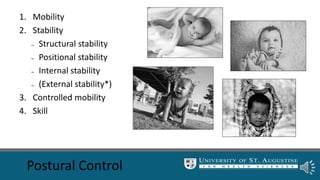
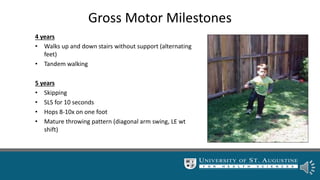
Motor development in children follows a generally predictable sequence, progressing from primitive reflexes in newborns to independent walking and running by age 2. Variability within and between children is normal and allows for exploration, but atypical development may show less variability and delays in achieving milestones. The focus of intervention is to provide varied experiences that expand a child's motor strategies and skills based on their readiness.