Downloaded 23 times








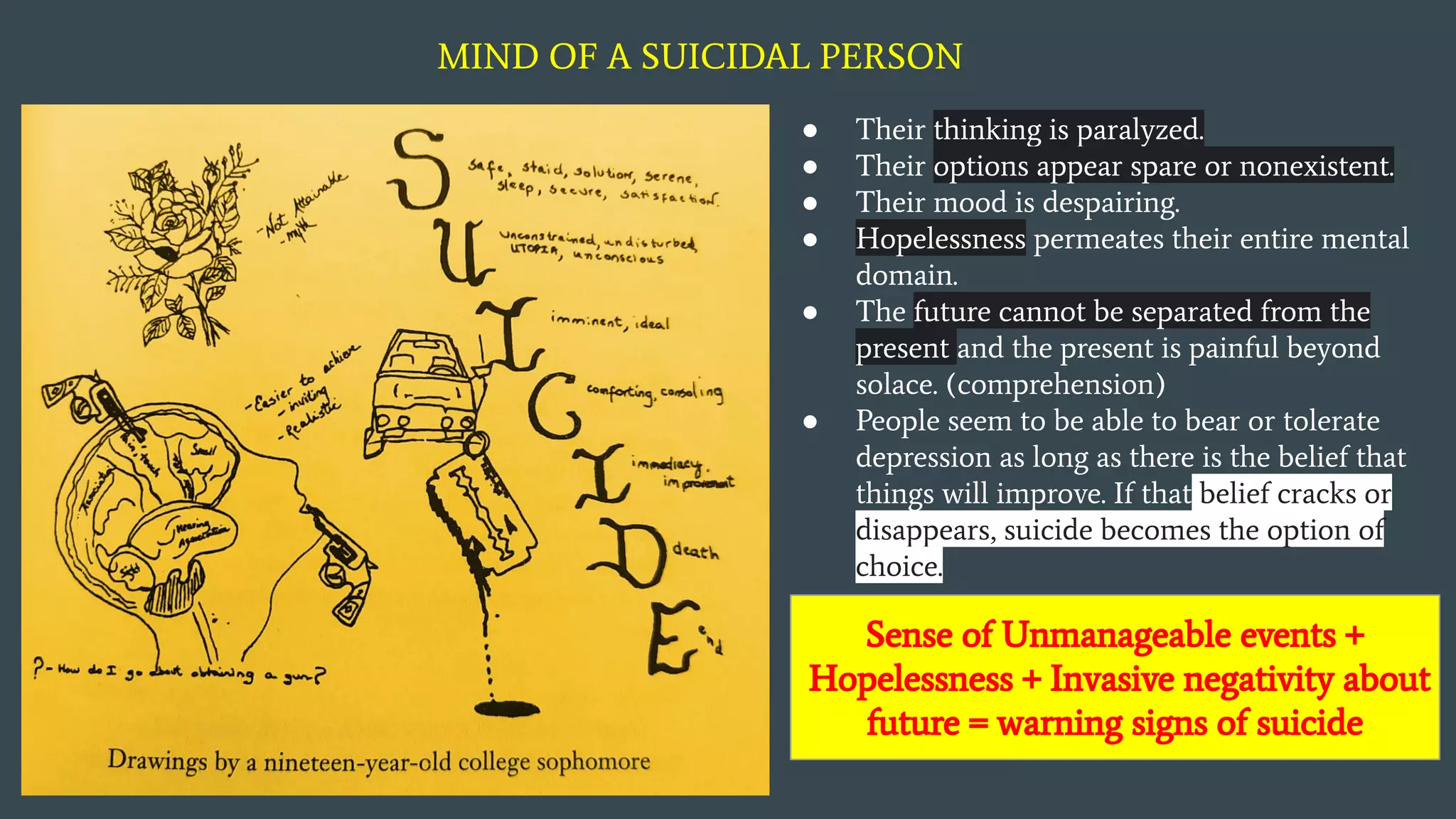

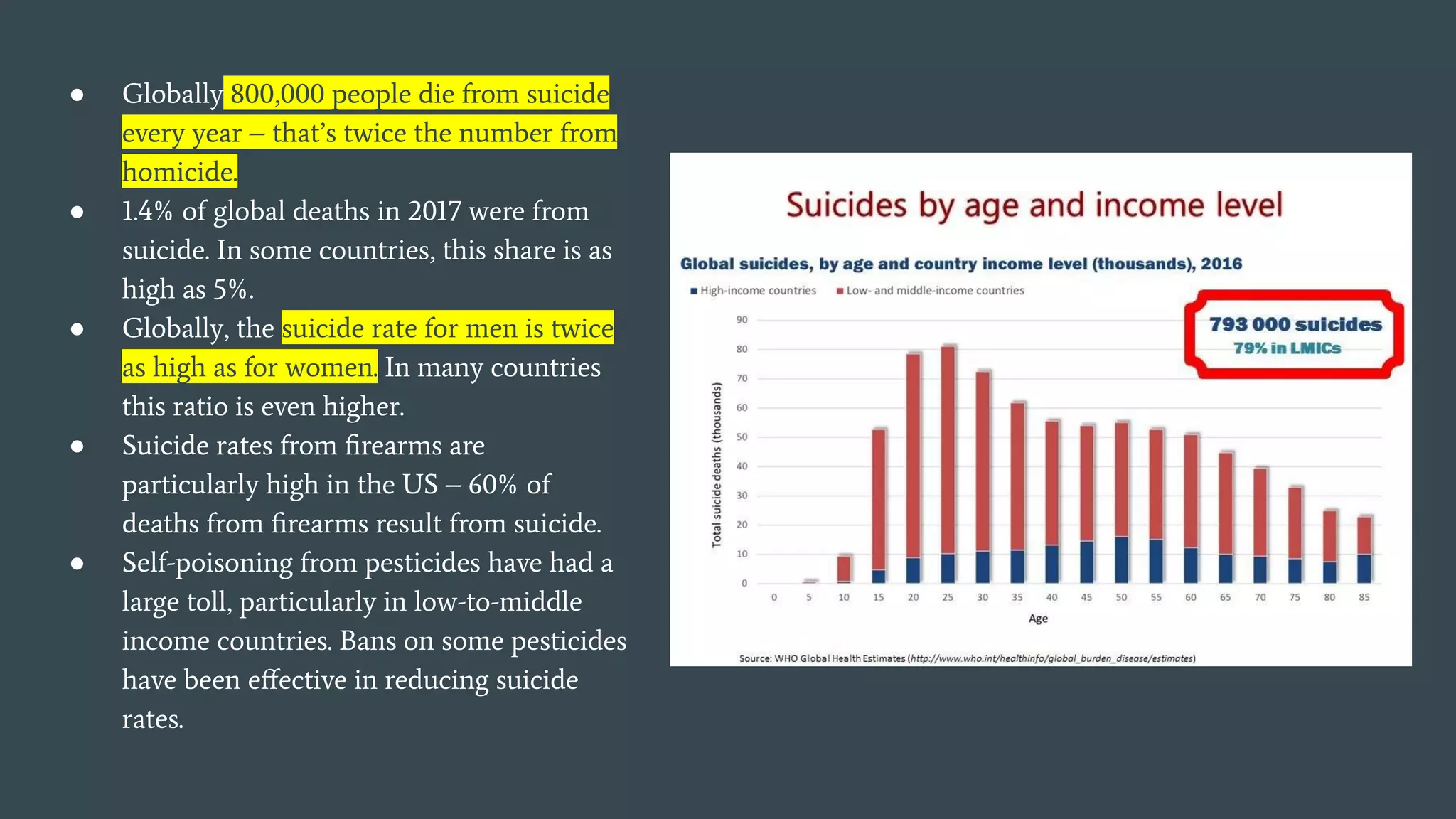











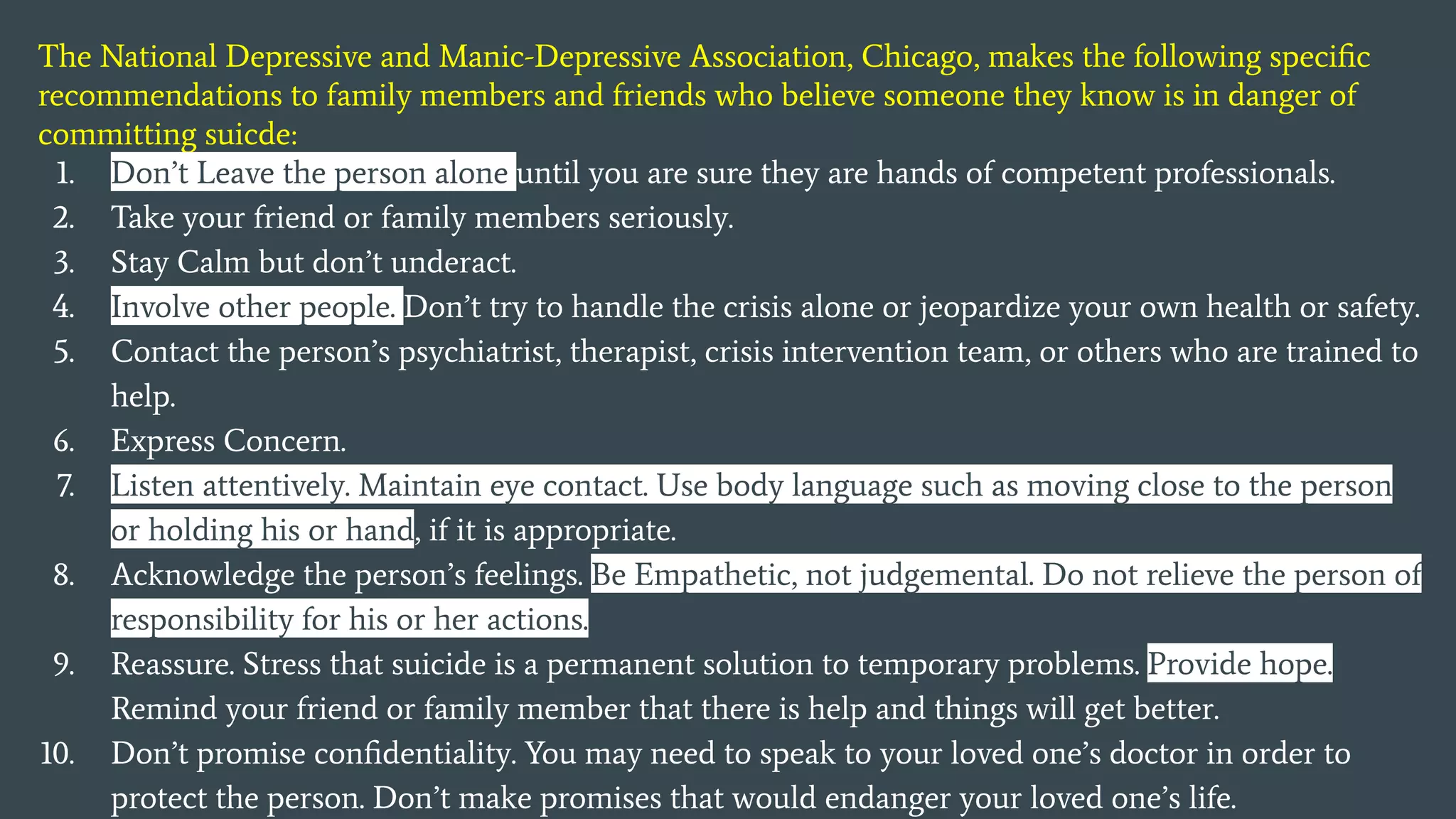






The document explores the complexities of suicide, defining it as a self-inflicted death often stemming from mental illness, despair, and societal pressures. It highlights the prevalence of suicidal ideation, particularly among youth, and examines factors influencing suicidal thoughts and behaviors, such as family dynamics and access to resources. Additionally, it discusses the role of media in shaping perceptions of suicide and the need for crisis intervention and mental health support in vulnerable populations.



































































