Downloaded 55 times





















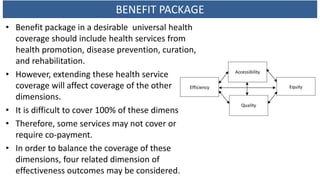






















![Adequate public
investment in health
• four Goals of SAFE
• Total health
expenditure (THE) is
not less than the
status quo level of
4.6 % of GDP (NHA
2013)
• GGHE as % of GGE is
not less than the
status quo level at
17% of GGE (NHA
2013)
GNI: Gross National Income, GDP: Gross Domestic Product, THE: Total Health Expenditure, GGHE: General
Government Health Expenditure,
GGE: General Government Expenditure, OOP: Household Out of pocket payment
GNI per capita,
US$
THE, %
GDP
THE per
capita, US$
GGHE %
THE
GGHE %
GGE
OOP %
THE
Reference year 2105 2014 2014 2014 2014 2014
Cuba
5,984
(2013)
11.1 817 95.6 18.0 4.4
France 30,404 11.5 4,959 78.2 15.7 6.3
Japan 28,099 10.2 3,703 83.6 20.3 13.9
Republic of Korea 21,835 7.4 2,060 54.1 12.3 36.1
Mexico 7,836 6.3 677 51.8 11.6 44
Norway 61,977 9.7 9,522 85.5 18.2 13.6
Thailand 4,350 4.1 228 77.8 13.2 11.9
European Union 26,517 10.0 3,613 77.8 16.0 13.9
Upper middle income country 6,362 6.2 NA 55.0 NA 36.2
High income country group 33,537 12.3 5,266 62.3 17.9 13.3
East Asia and Pacific
(all income level)
7,539 6.9 640 66.0 NA 25.2
Source: World Development Indicators, update 15 September 2017 [access 28 December 2017]
6-Jun-18 46](https://image.slidesharecdn.com/uhclessonlearn-180606011411/85/UHC-lesson-learn-Thailand-46-320.jpg)












The document discusses Thailand's universal health coverage (UHC) system, highlighting its principles, experiences, successes, and challenges. It covers the right to health, investment in health systems, and the historical development of healthcare financing in Thailand, emphasizing the importance of equitable access to health services. Despite the significant progress made, the document also addresses ongoing challenges, such as fiscal realities and the need for sustainable funding.










![Health care delivery system in Pakistan [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/healthcaredeliverysysteminpakistanautosaved-220516171858-8fd14214-thumbnail.jpg?width=640&height=640&fit=bounds)












































































