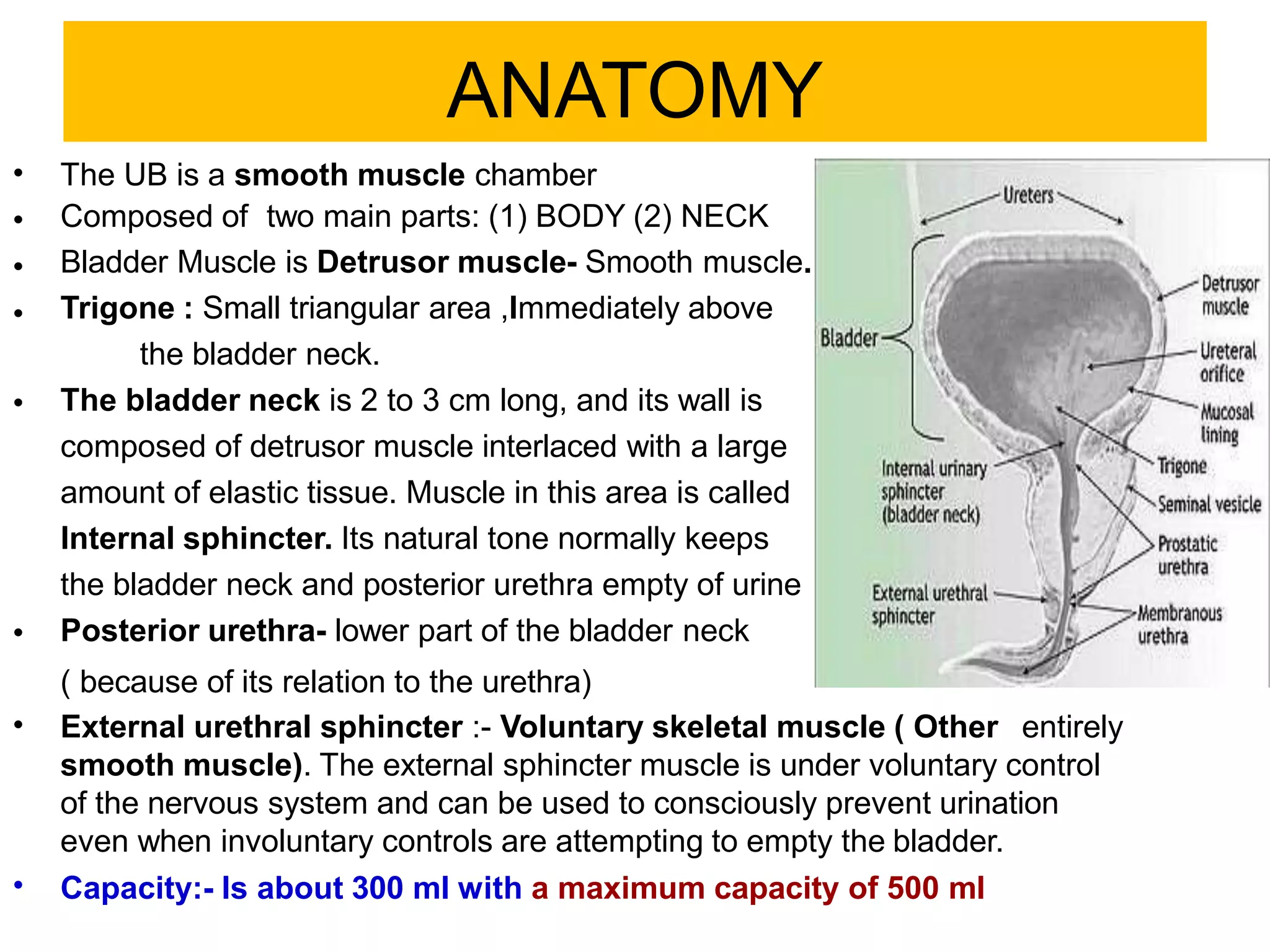
The document covers the anatomy, physiology, and neurobiology of the urinary bladder, detailing its functions, common disorders, and types of neurogenic bladder dysfunction. It emphasizes the importance of early intervention in preventing damage caused by high bladder pressures and summarizes complex neural control related to micturition. Additionally, it categorizes various types of urinary incontinence and their underlying causes, providing a comprehensive overview of bladder-related health issues.