Downloaded 91 times


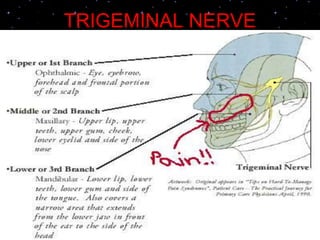
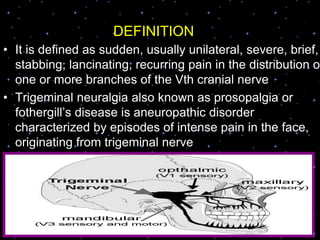
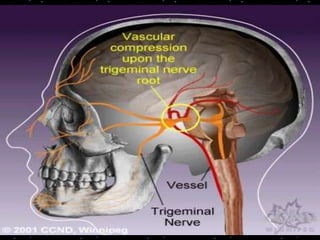

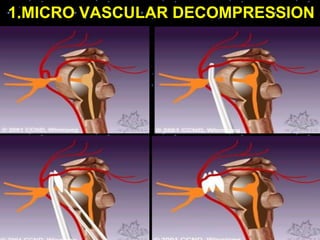
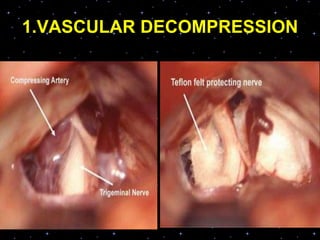
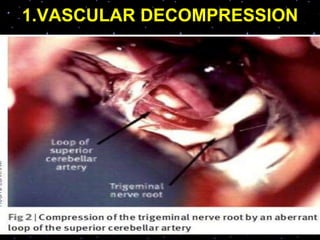
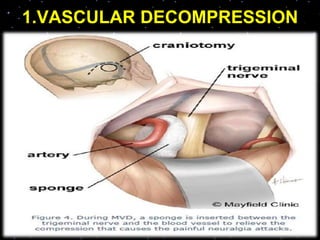


Trigeminal neuralgia is a severe facial pain disorder affecting the trigeminal nerve, the largest nerve in the face. It causes sudden, severe, electric shock-like pain in the areas of the face served by the trigeminal nerve. Trigeminal neuralgia is often triggered by normal activities like eating or talking. It is treated initially with medications like carbamazepine, but patients may require surgical treatments like microvascular decompression if medications do not help. Nursing care focuses on preventing pain triggers and providing psychological support for patients suffering from this debilitating disorder.


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








