The document provides a comprehensive overview of the trigeminal nerve, including its anatomical structure, divisions, and functions, particularly in relation to sensory and motor activities of the face. It discusses clinical examination methods, significance of injury to the nerve, associated disorders like trigeminal neuralgia, and treatment options. The importance of understanding the trigeminal nerve's anatomy is emphasized for effective diagnosis and management of related conditions.






















![33
Tic douloureux, or Trigeminal Neuralgia
• Frequent cause of facial pain.
• Paroxysmal pain of great intensity that involves any or all of the trigeminal division.
More frequent in the maxillary or mandibular division.
• Nature of pain- sudden, severe, brief, stabbing, recurrent pain, electric shock like
lancinating, burning, excruciating.
• Pain in areas supplied by the trigeminal nerve, including the cheek, jaw, teeth, gums,
lips, or less often the eye and forehead.
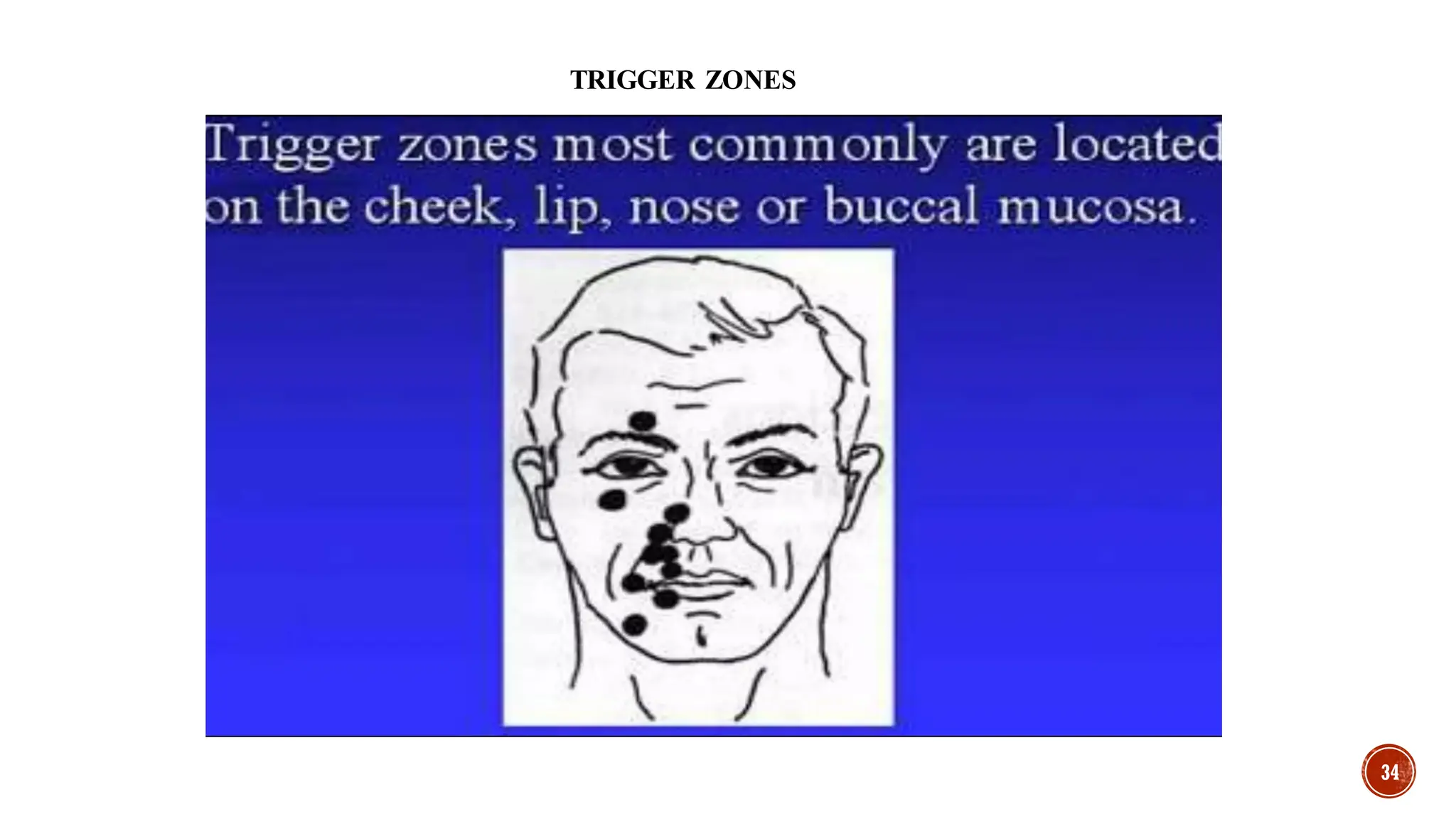
• A variety of triggers may set off the pain of trigeminal neuralgia, including : Shaving,
Touching your face, Eating, Drinking, Brushing your teeth, Talking, Putting on
makeup, Breeze lightly blowing over your face, Smiling, Washing your face
Shankar Kikkeri N, Nagalli . Trigeminal Neuralgia. [Updated 2022 Jul 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan](https://image.slidesharecdn.com/trigeminalnerve-250119165432-cc204afd/75/TRIGEMINAL-NERVE-Neuralgia-5th-cranial-nerve-33-2048.jpg)


![38
Drug therapy
• Carbamazepine is a gold standard as first line of therapeutic agent. Side
effect drowsiness, dizziness, double vision, and nausea.
• Adults—At first, 200 milligrams (mg) once a day. Your doctor may increase your dose as
needed and tolerated. However, the dose is usually not more than 1200 mg per day.
• Children—Use and dose must be determined by your doctor.
• Oxcarbazepine is a newer drug and is being increasingly used as first-line therapy for TN
in patients who do not respond to or who cannot tolerate carbamazepine. 150mg twice daily
upto max dosage of 1800mg/day
• Baclofen is a muscle relaxant that can be used to treat TN.10-20 mg/day upto max dosage
of 60-80 mg/day
• All above drugs are not in use now because of their side – effects.
• Nowadays Gabapentin is used. 300m/day upto 1800 mg/day
• Huff T, Weisbrod LJ, Daly DT. Neuroanatomy, Cranial Nerve 5 (Trigeminal) [Updated 2022 Nov 9]. In: StatPearls [Internet]. Treasure Island (FL):StatPearls Publishing; 2022 Jan.](https://image.slidesharecdn.com/trigeminalnerve-250119165432-cc204afd/75/TRIGEMINAL-NERVE-Neuralgia-5th-cranial-nerve-38-2048.jpg)

![40
References
• Vol 4, BD Chaurasia’s Human Anatomy Brain Neuroanatomy
• Textbook of clinical neuroanatomy by Vishram Singh
• Textbook of oral and maxillofacial Surgery by Neelima malik.
• Shankar Kikkeri N, Nagalli S. Trigeminal Neuralgia. [Updated 2022 Jul 9]. In: StatPearls[Internet].
Treasure Island (FL): StatPearlsPublishing; 2022 Jan.
• Huff T, Weisbrod LJ, Daly DT. Neuroanatomy, Cranial Nerve 5 (Trigeminal) [Updated 2022 Nov 9]. In:
StatPearls[Internet]. Treasure Island (FL): StatPearlsPublishing; 2022 Jan.
• Walker HK. Cranial Nerve V: The Trigeminal Nerve. In: Walker HK, Hall WD, Hurst JW, editors. Clinical
Methods:The History, Physical, and LaboratoryExaminations. 3rd edition. Boston:Butterworths; 1990.
Chapter61.
• International Journal of Clinical Pediatrics, ISSN 1927-1255print, 1927-1263online, Open Access
Article copyright, the authors; Journal compilationcopyright, Int J Clin Pediatr and Elmer Press Inc
Journal website http://www.theijcp.org](https://image.slidesharecdn.com/trigeminalnerve-250119165432-cc204afd/75/TRIGEMINAL-NERVE-Neuralgia-5th-cranial-nerve-40-2048.jpg)





























![ceph_LLP_SEMINAR[2].pptx landmarks lines and planes](https://cdn.slidesharecdn.com/ss_thumbnails/cephllpseminar2-250919182304-905904ac-thumbnail.jpg?width=640&height=640&fit=bounds)




























