Contents
Introduction
Function
Embryology
Musculature of the first pharyngeal arch
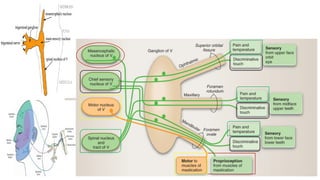
Nuclei of trigeminal nerve
Course
Trigeminal Ganglion
Branches
Ophthalmic Nerve
Maxillary Nerve
Mandibular Nerve
Applied anatomy
3.
Introduction
Trigeminal nerve isthe largest cranial
nerve.
It is a mixed nerve.
It is composed of a small motor root and a
considerably larger sensory root.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Function
The sensoryfunction of the trigeminal nerve is
to provide the tactile, proprioceptive, and
nociceptive afference of the face and mouth.
The motor function activates the muscles of the
mastication, the tensor tympani, tensor veli
palatini, mylohyoid, and anterior belly of the
digastric.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
6.
Embryology
of the nerve
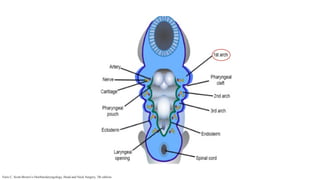
During the development of embryo, the
pharyngeal arches appear in the fourth and fifth
week.
It give rise to six pharyngeal arches, of which
the 5th
arch disappears.
Trigeminal nerve is derived from 1st
pharyngeal
arch
Musculature
of the first
pharyngeal
arch
Muscles of mastication :Temporalis, Masseter,
Pterygoids
Anterior belly of digastric
Mylohyoid
Tensor tympani
Tensor veli palatini
The nerve supply to these muscles is provided by mandibular
division of trigeminal nerve.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
9.
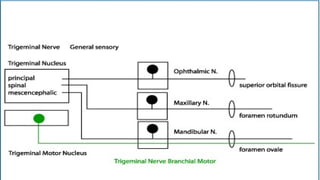
Nuclei of
trigeminal
nerve
Mesencephalicnuclei (midbrain)
Main sensory nuclei (upper pons)
Motor nuclei (upper pons)
Spinal nuclei (upper pons to C2 segment of
spinal cord)
Faris C. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery, 7th edition.
11.
Course
The trigeminalnerve exits from the anterolateral
surface of the pons as a large sensory root and a small
motor root.
These roots continue forward out of the posterior
cranial fossa and into the middle cranial fossa by
passing over the medial tip of the petrous part of the
temporal bone.
Faris C. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery, 7th edition.
12.
Course
In themiddle cranial fossa the sensory root expands
into the trigeminal ganglion.
The ganglion is in a depression (the trigeminal
depression) on the anterior surface of the petrous part
of the temporal bone, in a Dural cave (the Meckel’s
cave).
The motor root is below and completely separate from
the sensory root at this point.
Faris C. Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery, 7th edition.
Course
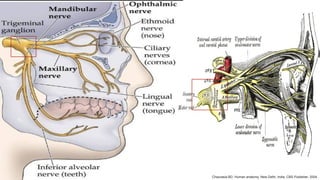
From theanterior border of the trigeminal
ganglion are the three terminal divisions of the
trigeminal nerve which are Ophthalmic (V1),
Maxillary (V2), and Mandibular (V3).
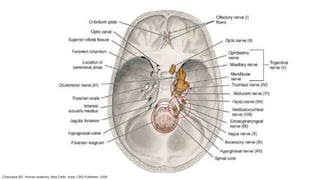
Fibers run from the pons to the face -
1. via the Superior Orbital Fissure (V1),
2. the foramen Rotundum (V2),
3. the foramen Ovale (V3)
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Trigeminal
Ganglion
Also knownas- Gasserian ganglion,
or Semilunar ganglion.
It is a sensory ganglion of the trigeminal nerve
that occupies a cavity (Meckel's cave) in the
dura mater.
It covers the trigeminal impression near the
apex of the petrous part of the temporal bone.
The central processes of the ganglion cells
form the large sensory root of the trigeminal
nerve, which is attached to pons at its junction
with the Middle cerebellar peduncle.
The peripheral processes form the three
divisions of the trigeminal nerve.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Ophthalmic
Nerve
It isthe superior and the smallest division.
It is a sensory nerve.
It communicates with the oculomotor, trochlear
and abducent nerve.
The latter communication may be the route by
which proprioceptive fibers from extraocular
muscles enter the trigeminal nuclear complex.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
22.
Ophthalmic
Nerve
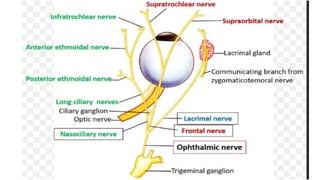
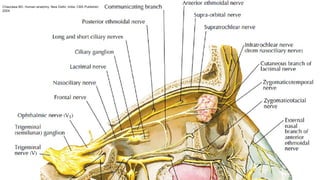
Before enteringthe orbit by the superior orbital
fissure it divides into- Lacrimal (smallest),
Nasociliary (intermediate), Frontal (largest).
Nasociliary divides into Internal nasal, External
nasal.
External nasal further divides into Long ciliary,
Infra Trochlear, Posterior Ethmoidal.
Frontal divides into Supra Trochlear, Supra
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Maxillary
Nerve
It isintermediate division of trigeminal nerve.
It is completely sensory.
Course-
It leaves the trigeminal ganglion between the
ophthalmic and mandibular divisions as a flat
plexiform band.
It passes slightly medial to lateral wall of
cavernous sinus.
It leaves the cranium through foramen
rotundum, which is located in the greater wing
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Maxillary
Nerve
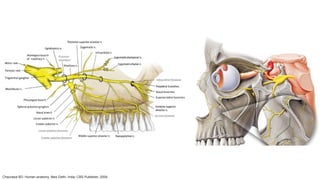
The maxillarydivision emerges on the anterior
surface of face through the infraorbital
foramen, where it divides into its terminal
branches, supplying the skin of the face, nose,
lower eyelid and upper lip.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
29.
Mandibular
Nerve
A Smallmotor root which passes under the
ganglion to unite with the sensory root just
outside the skull.
A Large Sensory root which arises from lateral
part of trigeminal ganglia in middle cranial
fossa.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Mandibular
Nerve
The teethand gums of the mandible.
The skin in the temporal region, part of the
auricle, including the external meatus and
tympanum.
The lower lip, the lower part of the face.
The muscles of mastication.
The mucosa of the anterior two-thirds of the
tongue and the mucosa of the floor of the oral
cavity.
Chaurasia BD. Human anatomy. New Delhi, India: CBS Publisher; 2004.
Trigeminal
neuralgia
Also knownas Fothergill’s disease/ Tic douloureux
(painful jerking)
It is defined as sudden, usually unilateral, severe, brief,
stabbing, lancinating, recurring pain in the distribution
of one or more branches of trigeminal nerve.
Mean age: 40-50 years onwards with Female
predominance. (male : female = 1:2 ~2:3)
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
36.
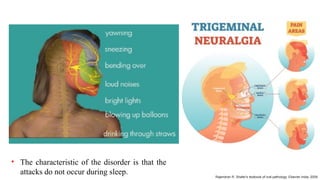
• The characteristicof the disorder is that the
attacks do not occur during sleep. Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
37.
Trigeminal
neuralgia
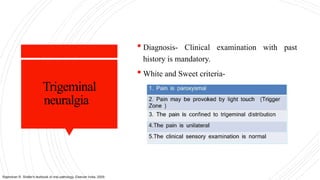
Diagnosis- Clinicalexamination with past
history is mandatory.
White and Sweet criteria-
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
38.
Trigeminal
neuralgia
Treatment
Primary management-
Carbamazepine(Tegretol) 100 mg
Percutaneous management-
Injection of 60% to 90% alcohol/ percutaneous
glycerol in the nerve trunk or ganglion.
Radiofrequency ablation.
Surgical management-
Peripheral neurectomy
Gasserian ganglion procedures
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
39.
Herpes zoster
ophthalmicus
Causedby Varicella zoster
Predilection for nasociliary branch of ophthalmic
division of the trigeminal nerve.
Clinical features:-
Cutaneous lesions:-
Rash
Vesicle
Pustule crust permanent scar
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
Herpes zoster
ophthalmicus
Treatment:-
Acyclovir800mg 5 times/ day within 4 days of
onset of rash
Analgesics
Antibiotic ointments
Systemic steroids 60mg/day
Corneal grafting
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
43.
Wallenberg
Syndrome
Also knownas Posterior inferior cerebellar
artery syndrome (PICA) or Lateral medullary
syndrome.
A stroke which causes loss of pain/temperature
sensation from one side of the face and
the other side of the body.
Etiology:
In the medulla, the Ascending Spinothalamic
Tract (which carries pain/temperature
information from the opposite side of the body) is
adjacent to the Descending Spinal Tract of the
fifth nerve (which carries pain /temperature
information from the same side of the face).
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
44.
Wallenberg
Syndrome
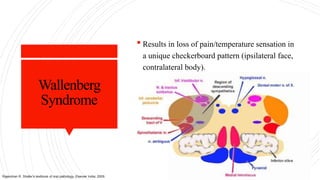
Results inloss of pain/temperature sensation in
a unique checkerboard pattern (ipsilateral face,
contralateral body).
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
45.
Mental nerve
neuralgia
Dueto resorption of the lower alveolar ridge,
the borders of the denture flange may compress
the mental nerve causing pain.
Radiographically, the foramen can be seen at
the level of the surface of the ridge.
Similar pain can be felt due to narrowing of the
foramen.
Treatment
Shifting of the foramen down is the treatment
of choice.
Decompression of the nerve by enlarging the
canal.
Malik NA. Text Book of Oral And Maxillofacial surgery.
46.
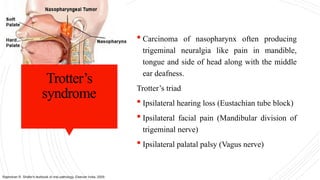
Trotter’s
syndrome
Carcinoma ofnasopharynx often producing
trigeminal neuralgia like pain in mandible,
tongue and side of head along with the middle
ear deafness.
Trotter’s triad
Ipsilateral hearing loss (Eustachian tube block)
Ipsilateral facial pain (Mandibular division of
trigeminal nerve)
Ipsilateral palatal palsy (Vagus nerve)
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
47.
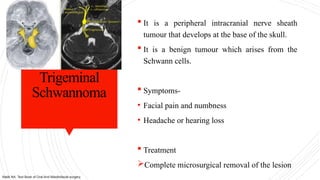
Trigeminal
Schwannoma
It isa peripheral intracranial nerve sheath
tumour that develops at the base of the skull.
It is a benign tumour which arises from the
Schwann cells.
Symptoms-
• Facial pain and numbness
• Headache or hearing loss
Treatment
Complete microsurgical removal of the lesion
Malik NA. Text Book of Oral And Maxillofacial surgery.
48.
Superior
orbital fissure
syndrome
Dueto dislocation of bony fragments or
comminute fracture in the region of superior
orbital fissure, a group of neurological deficit
expressed by altered functions of the nerves
passing through it.
It can also occur due to inflammation and
tumour.
Symptoms-
• Vision loss
• Periorbital pain
• Diplopia
• Lacrimal hyposecretions
Malik NA. Text Book of Oral And Maxillofacial surgery.
49.
Frey’s
syndrome
A conditionof localised gustatory sweating and
flushing of areas supplied by auriculotemporal
nerve (ATN).
Etiology-
Parotid gland or TMJ surgery
Facial wound or parotid abscess
Suppurative parotitis
Treatment-
Topical agents-Aluminium chloride hexahydrate
(Anti perspirant)
Radiation therapy
Rajendran R. Shafer's textbook of oral pathology. Elsevier India; 2009.
50.
Post surgical
complications
A3rd
molar impaction case may result in trauma
to lingual nerve, leading to loss of sensation to
the anterior of the tongue.
Trans antral procedure- Paraesthesia of the
upper lip, gums, and teeth.
Cancer surgeries- The tendency of squamous
cell carcinoma to effect the cutaneous branches
places these nerves at risk for injury during
surgery.
Malik NA. Text Book of Oral And Maxillofacial surgery.
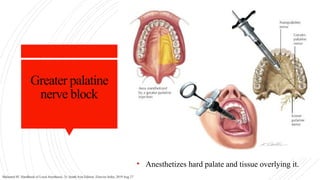
Greater palatine
nerve block
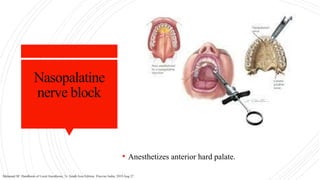
•Anesthetizes hard palate and tissue overlying it.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India; 2019 Aug 27.
53.
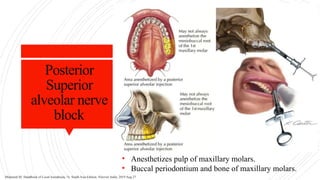
Posterior
Superior
alveolar nerve
block
• Anesthetizespulp of maxillary molars.
• Buccal periodontium and bone of maxillary molars.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India; 2019 Aug 27.
54.
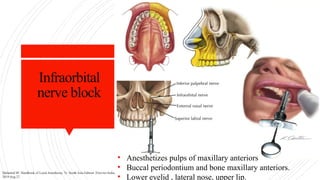
Infraorbital
nerve block
• Anesthetizespulps of maxillary anteriors
• Buccal periodontium and bone maxillary anteriors.
• Lower eyelid , lateral nose, upper lip.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India;
2019 Aug 27.
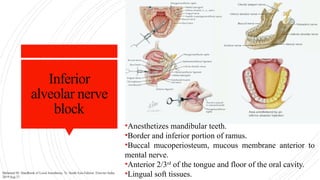
Inferior
alveolar nerve
block
•Anesthetizes mandibularteeth.
•Border and inferior portion of ramus.
•Buccal mucoperiosteum, mucous membrane anterior to
mental nerve.
•Anterior 2/3rd
of the tongue and floor of the oral cavity.
•Lingual soft tissues.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India;
2019 Aug 27.
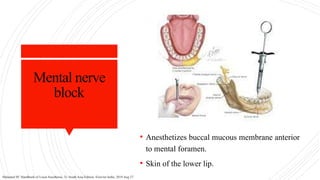
Mental nerve
block
• Anesthetizesbuccal mucous membrane anterior
to mental foramen.
• Skin of the lower lip.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India; 2019 Aug 27.
59.
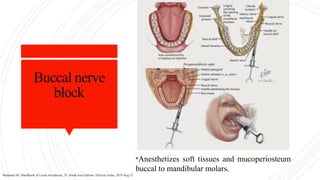
Buccal nerve
block
•Anesthetizes softtissues and mucoperiosteum
buccal to mandibular molars.
Malamed SF. Handbook of Local Anesthesia, 7e: South Asia Edition. Elsevier India; 2019 Aug 27.
60.
Conclusion
It isimportant that as dentists we should be
aware of the course and branches of trigeminal
nerve, to treat the patient with confidence, to
diagnose the pathological conditions and
moreover for the administration of local
anesthesia more efficiently without hurting the
patient and to prevent further complications.
61.
References
Chaurasia BD.Human anatomy. New Delhi, India:
CBS Publisher; 2004.
Malamed SF. Handbook of Local Anesthesia, 7e:
South Asia Edition. Elsevier India; 2019 Aug 27.
Rajendran R. Shafer's textbook of oral pathology.
Elsevier India; 2009.
Malik NA. Text Book of Oral And Maxillofacial
surgery.
Faris C. Scott-Brown’s Otorhinolaryngology, Head
and Neck Surgery, 7th edition.
Drake R, Vogel AW, Mitchell AW. Gray's anatomy
for students. Elsevier Health Sciences; 2009 Apr 4.
Tandon S. Textbook of pedodontics. Paras
medical publisher; 2009.




















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






