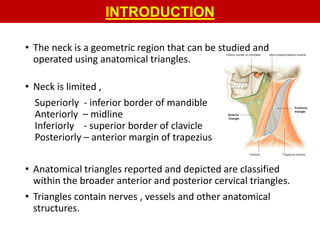
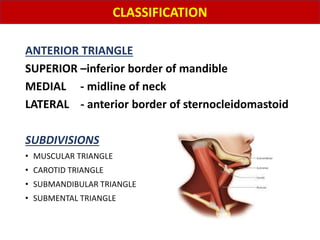
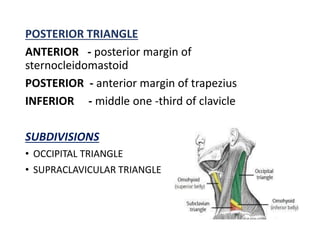
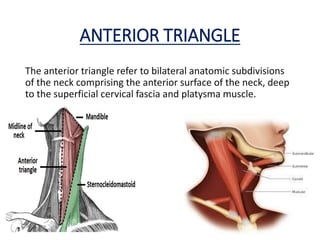
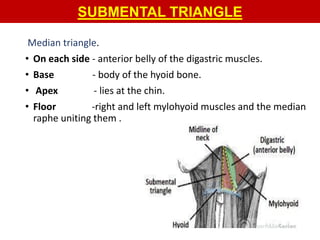
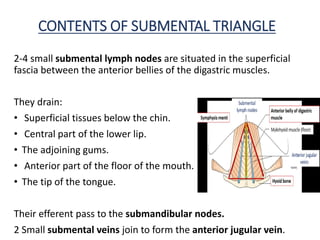
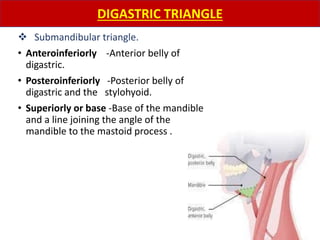
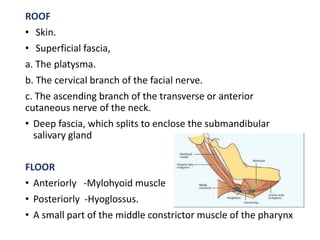
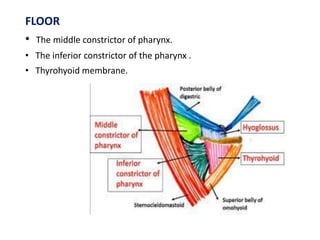
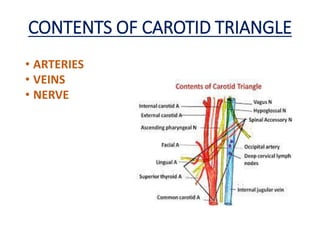
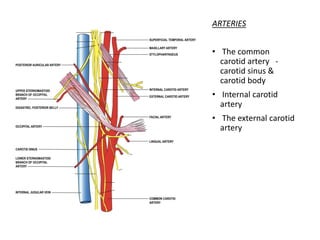
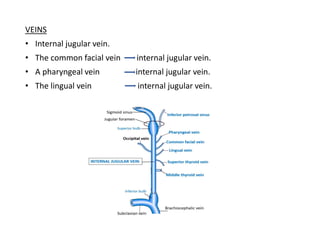
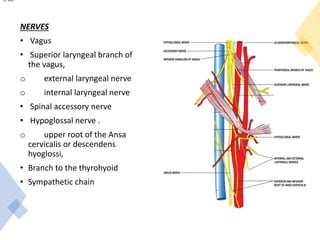
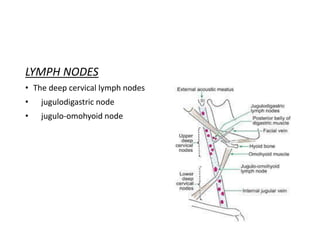
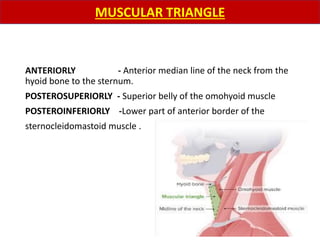
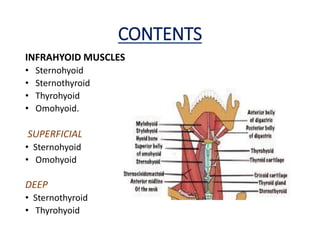
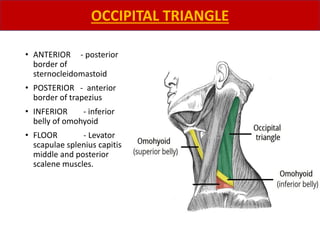
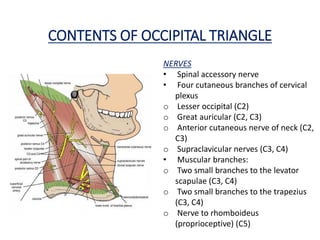
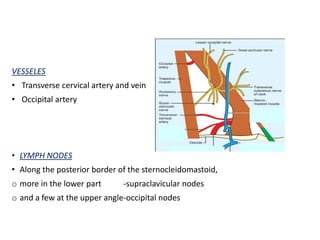
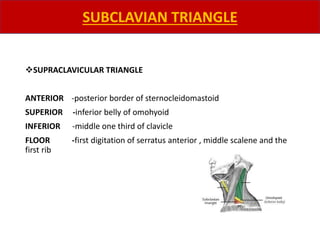
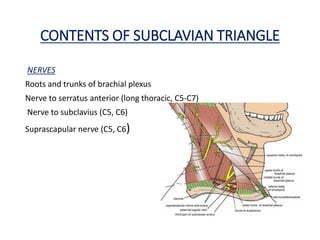
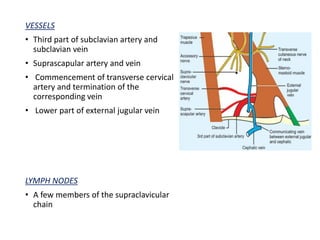
The document describes various anatomical triangles of the neck region. It discusses 11 triangles in detail, providing their boundaries, contents, and clinical significance. The triangles described include the anterior triangle, submental triangle, submandibular triangle, carotid triangle, muscular triangle, posterior triangle, occipital triangle, and supraclavicular triangle. Structures like nerves, vessels, muscles and lymph nodes contained within each triangle are outlined. Potential surgical and pathological implications are also mentioned.

























































![CPR AND EMERGENCY MEDICATIONS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cprandemergencymedicationsautosaved-250204082316-1c1ad7d9-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








