





























































































![3) Periodontal tissue consideration :
1]the width of the alveolus is usually in
sufficient for the roots of the teeth to pass
labio-palatally.
2) Root resorption may then occur as a
result of compression and friction during the
correction.
3) Thinning of the labial alveolus and
mucosa may result in clefting and recession
of the gingiva.
www.indiandentalacademy.com](https://image.slidesharecdn.com/transpositionofteethitsmanagement-140305001629-phpapp01/75/Transposition-of-teeth-its-management-102-2048.jpg)




















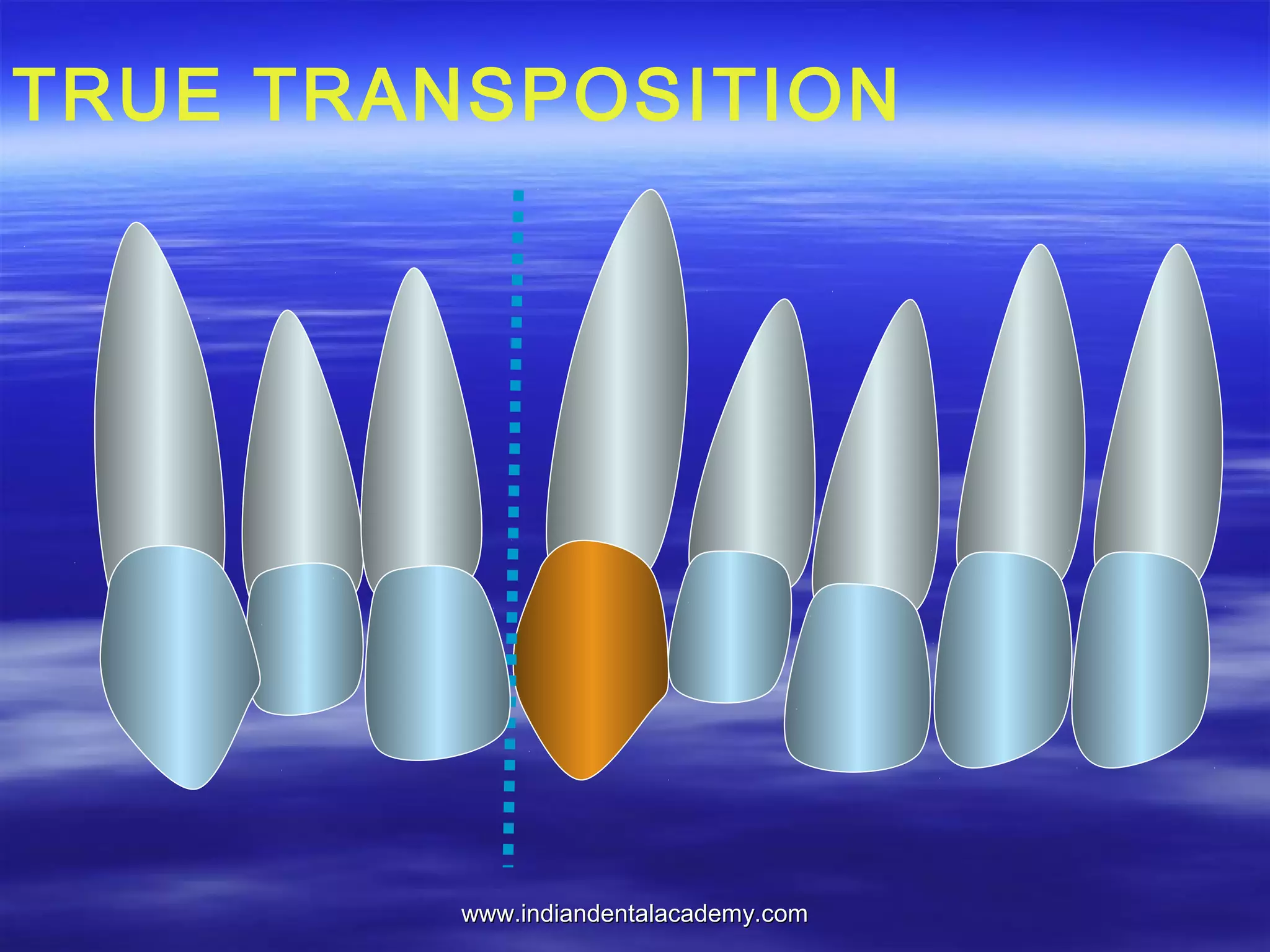
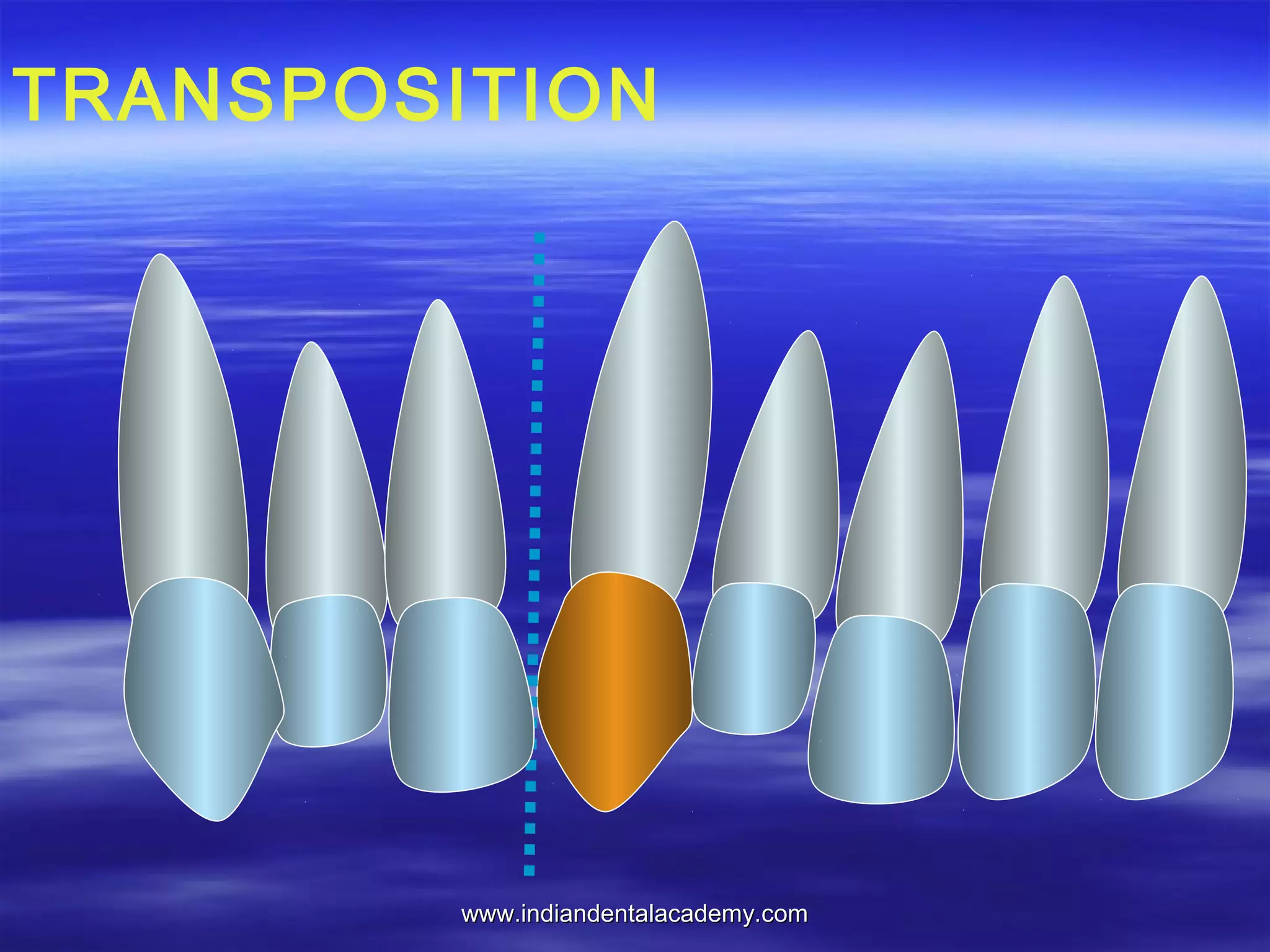
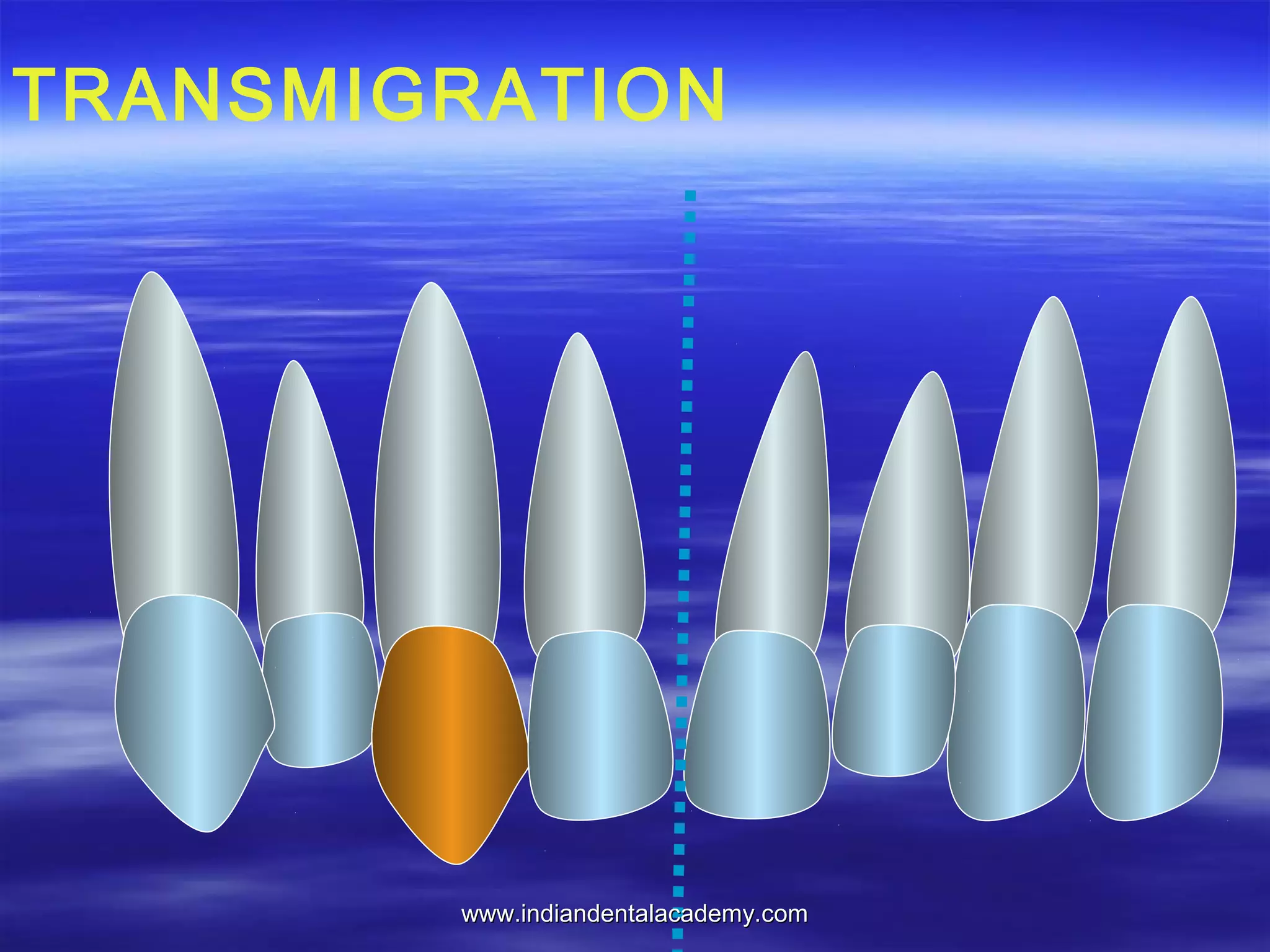
This document discusses the dental anomaly of tooth transposition. It begins with an introduction that defines transposition as the interchange of positions between two teeth. It then covers the history, definitions, classifications, controversies regarding etiology, clinical features, and management of tooth transposition. Key points include that maxillary canine to first premolar transposition is most common, transposition has been observed since the early 19th century, and the precise cause remains unknown but is likely genetic and multifactorial. Clinical management involves either interceptive treatment during development or definitive treatment after eruption.























































































