Downloaded 12 times



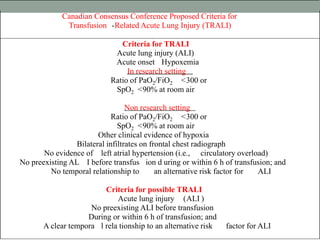




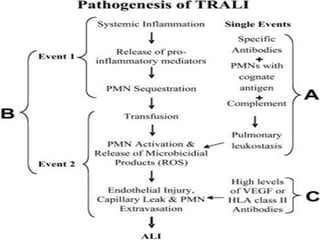




















Transfusion-related acute lung injury (TRALI) is a rare complication of blood transfusion characterized by acute lung injury within 6 hours of transfusion. It is difficult to diagnose due to a lack of clear defining criteria. Two mechanisms are proposed - antibodies in donor blood products cause activation of recipient neutrophils (single hit model) or antibodies interact with primed recipient neutrophils/pulmonary endothelium (two hit model). Risk factors include plasma-containing blood products from multiparous female donors or those stored for a long duration. Treatment involves stopping the transfusion and providing supportive care. Preventive strategies aim to reduce donor antibodies by excluding high-risk donors or using leukoreduction filters. TRALI must be differentiated from trans









































































