Download to read offline


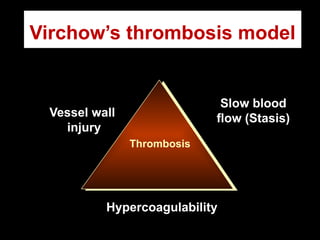
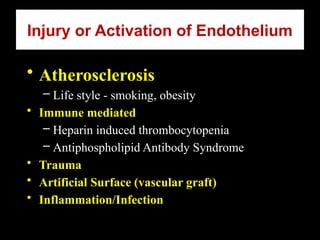
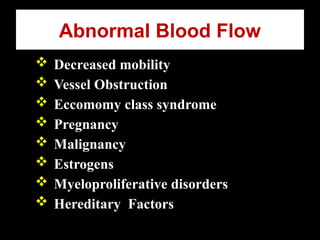
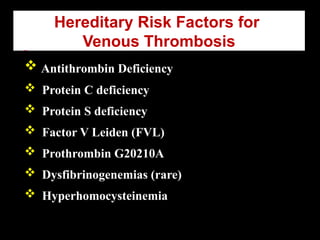
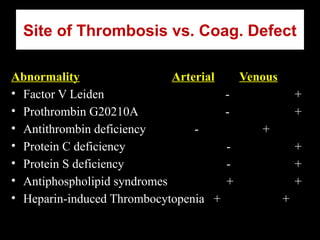




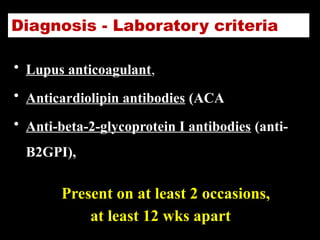

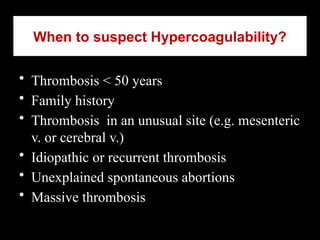
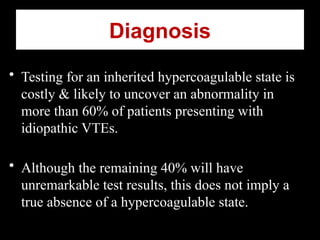



The document discusses hypercoagulable states, specifically thrombophilia, outlining its definition, mechanisms, and inherited conditions with clinical case studies. It emphasizes the necessity of recognizing risk factors, conducting appropriate tests, and managing patients effectively to prevent serious complications like venous thromboembolism. The cases highlight the importance of thrombophilia testing in certain patient profiles and the implications for long-term anticoagulation therapy.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











