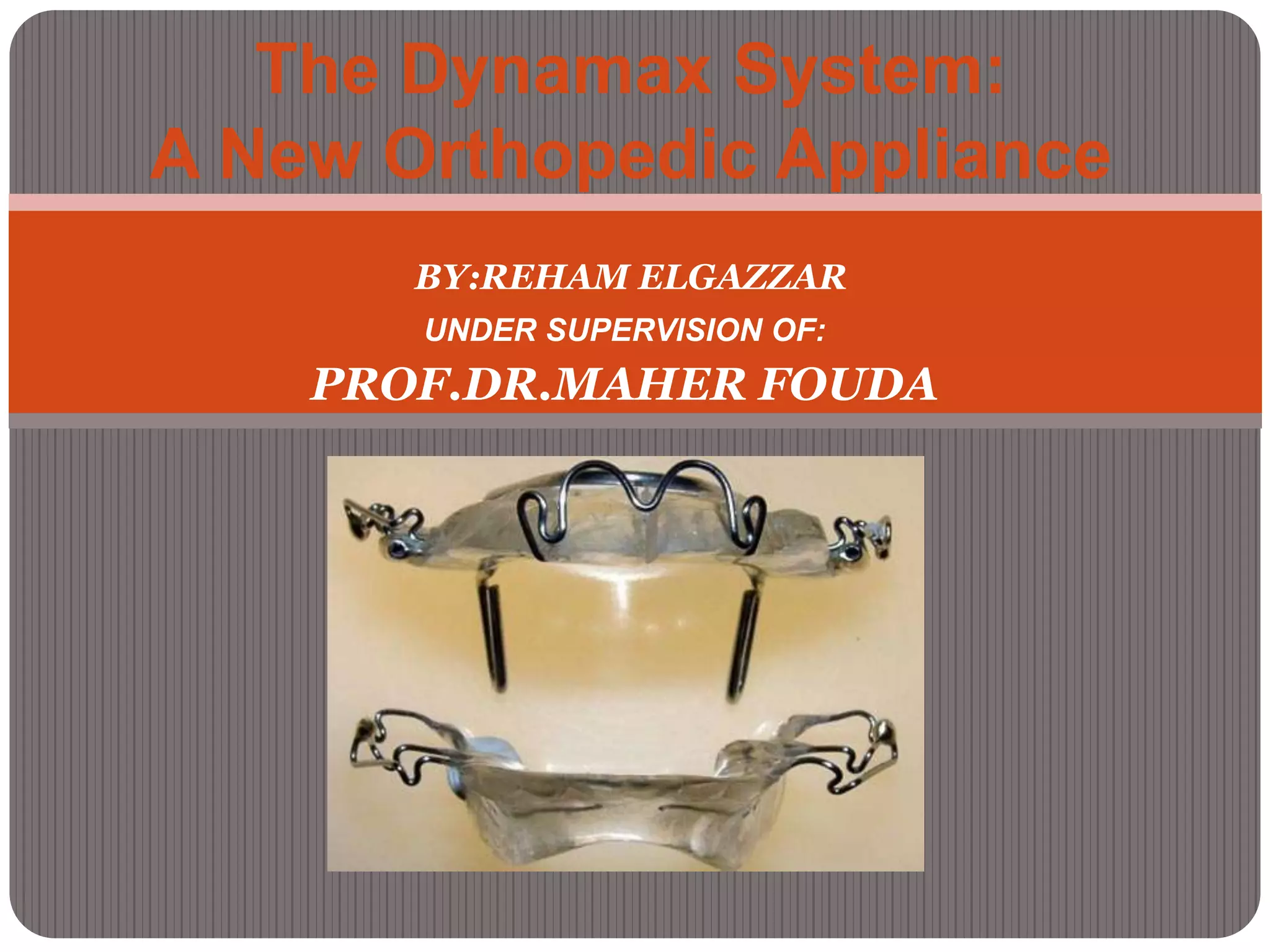
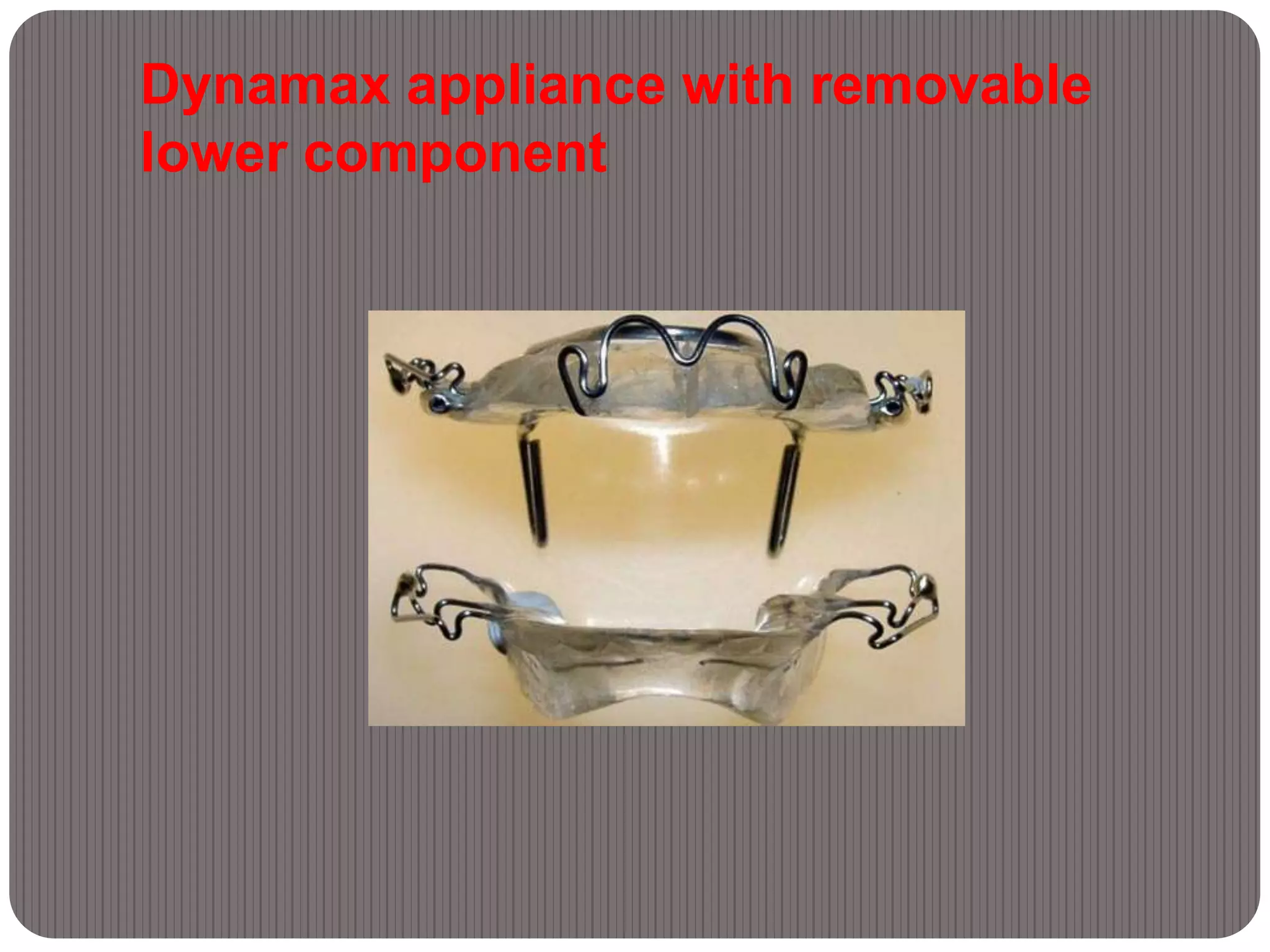
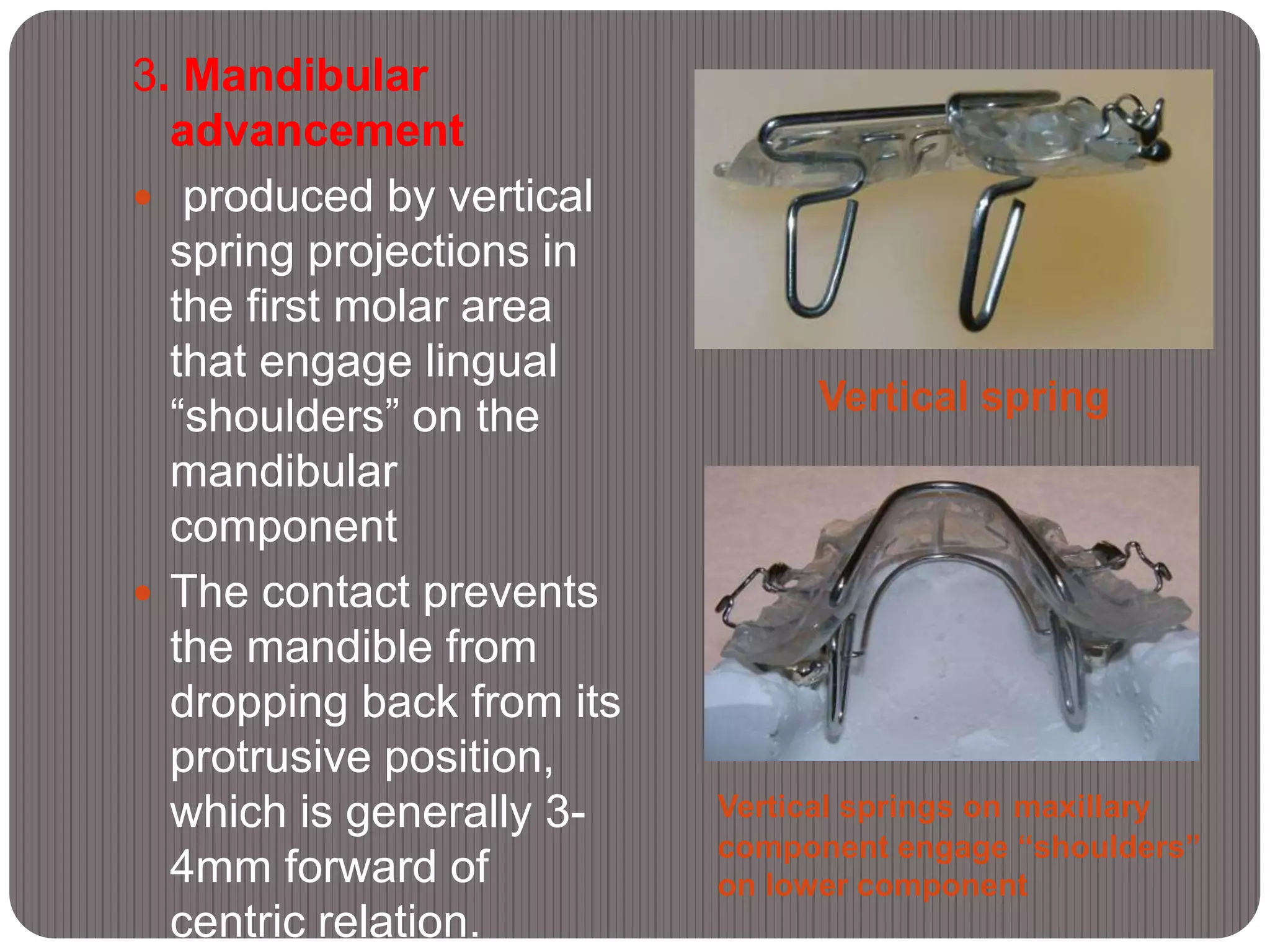
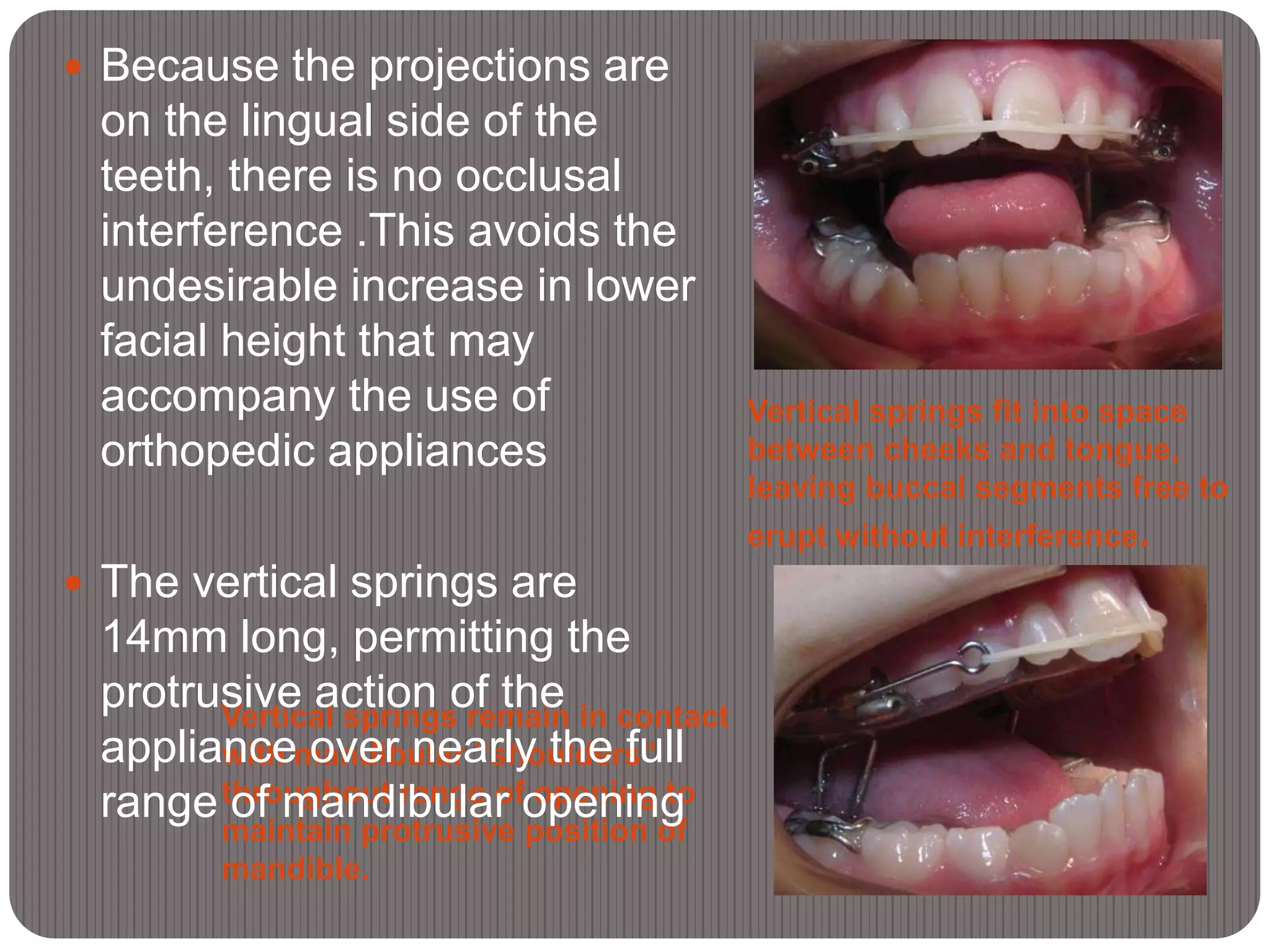
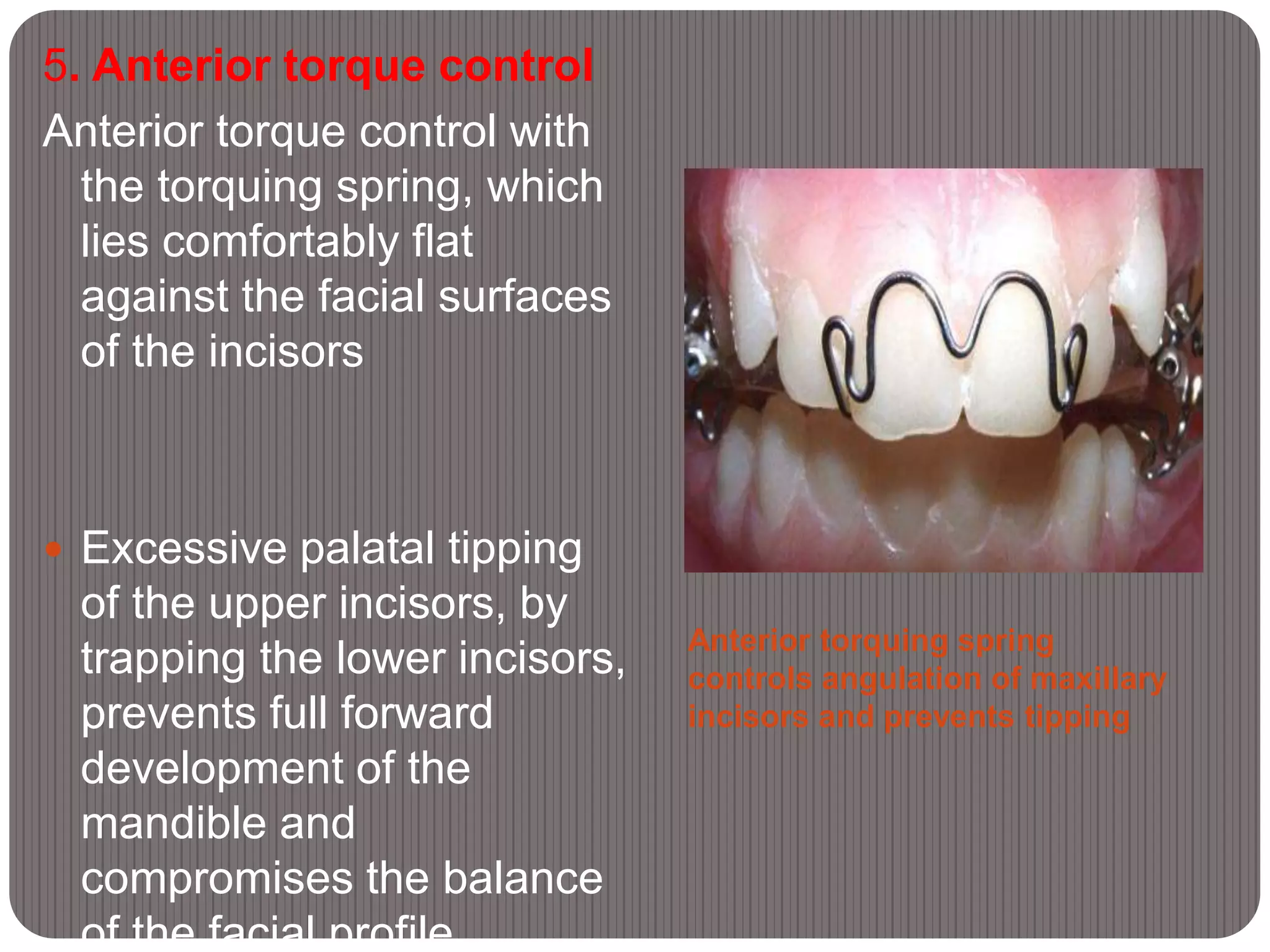
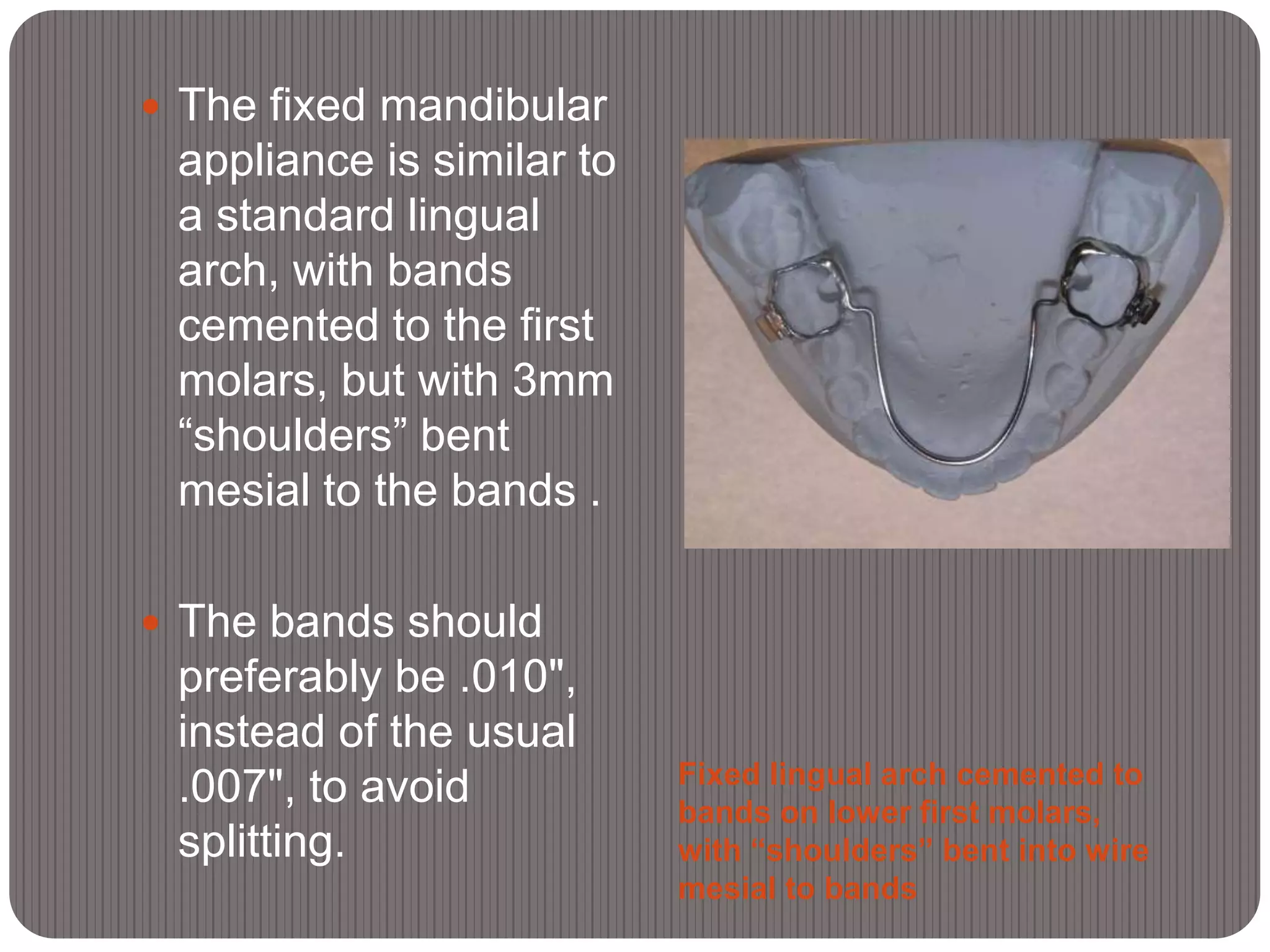
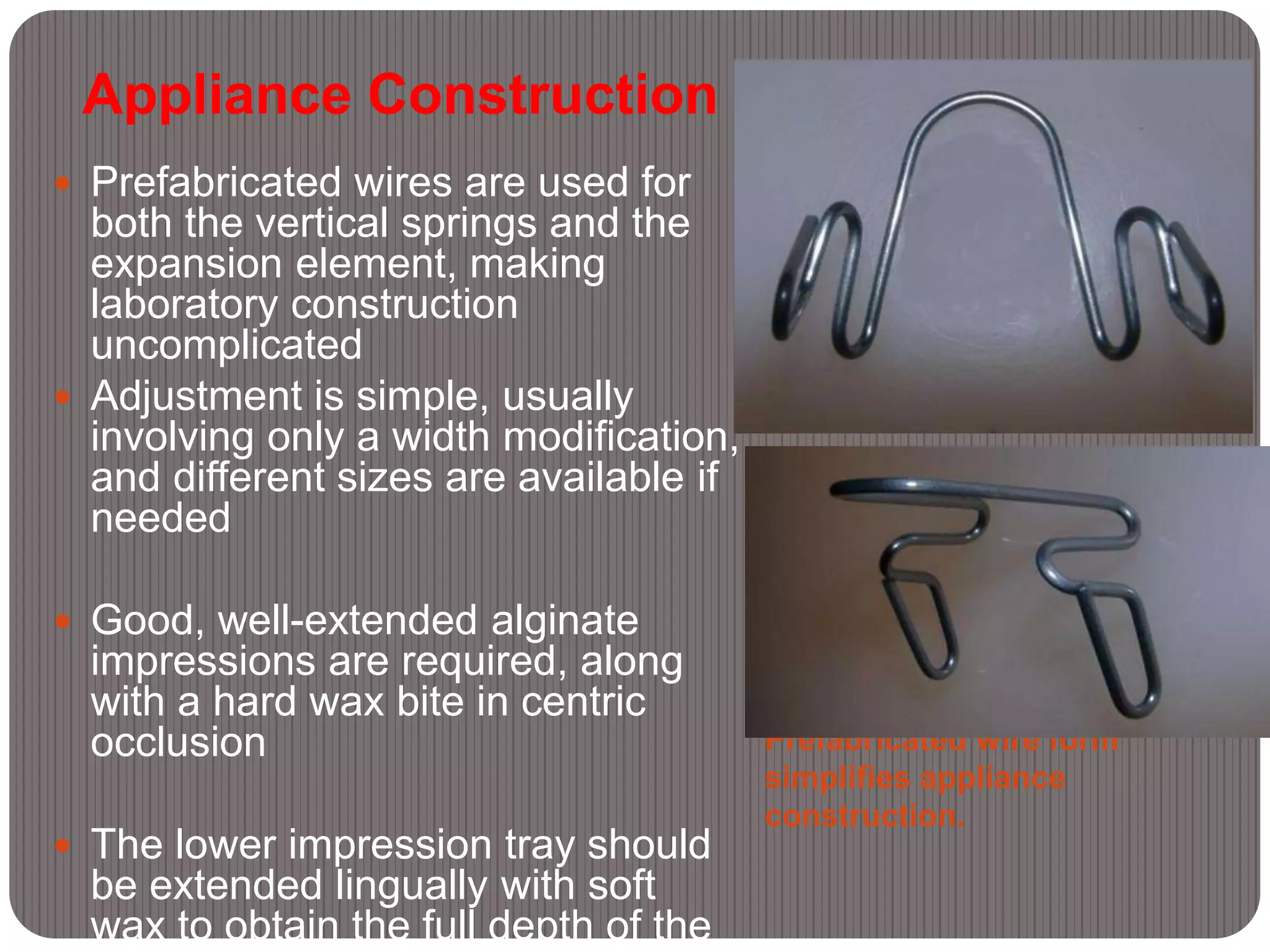
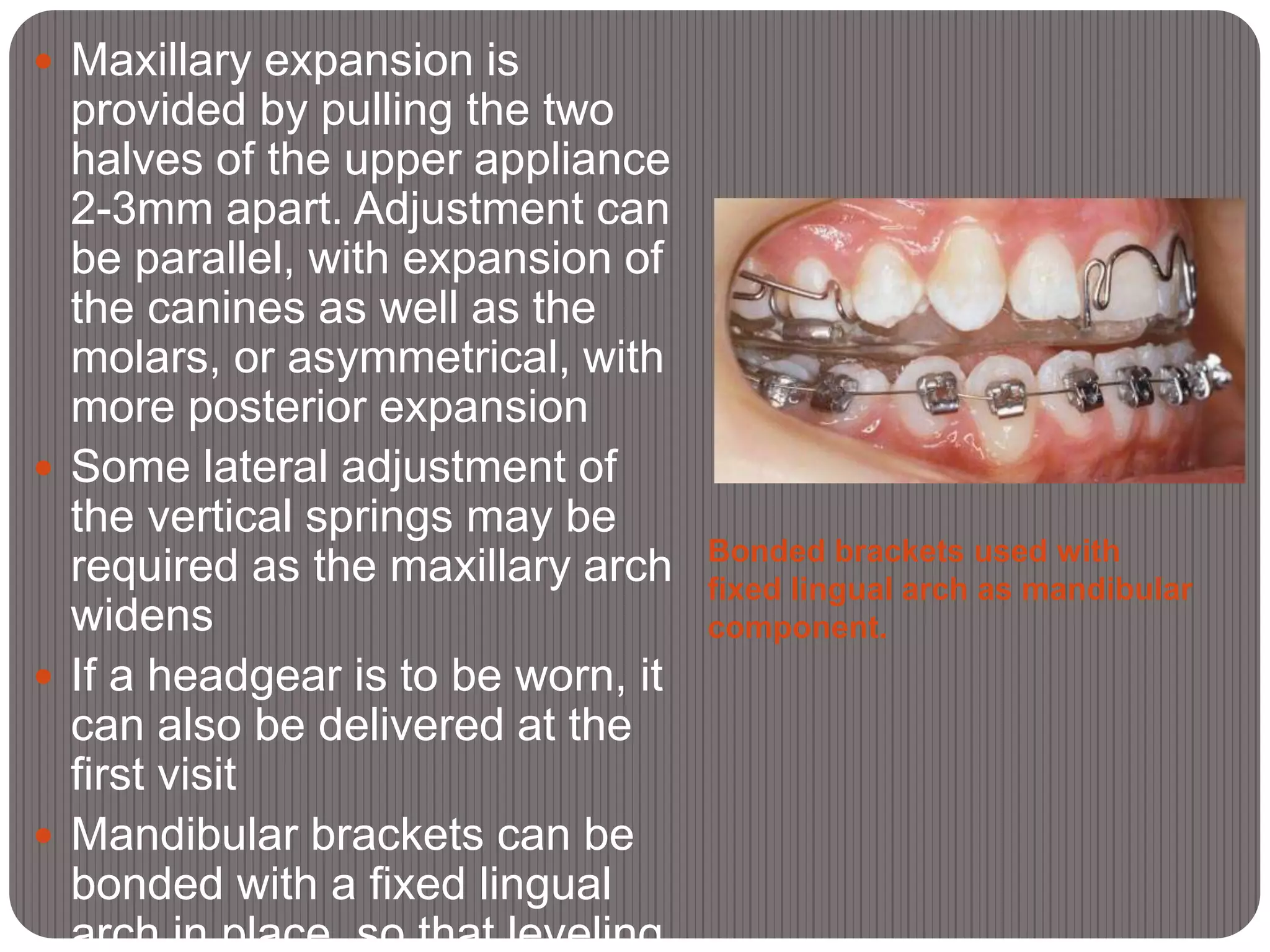
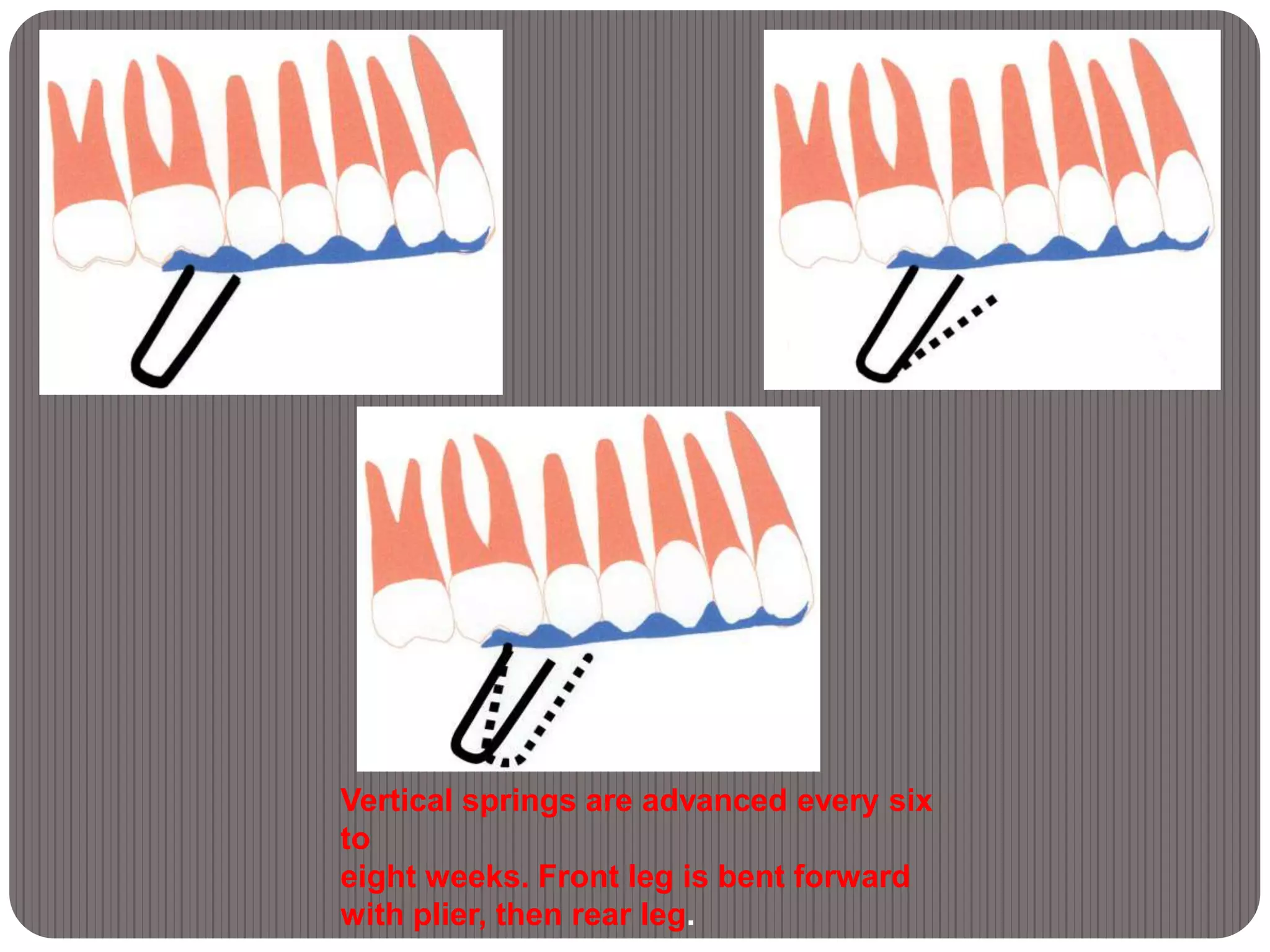
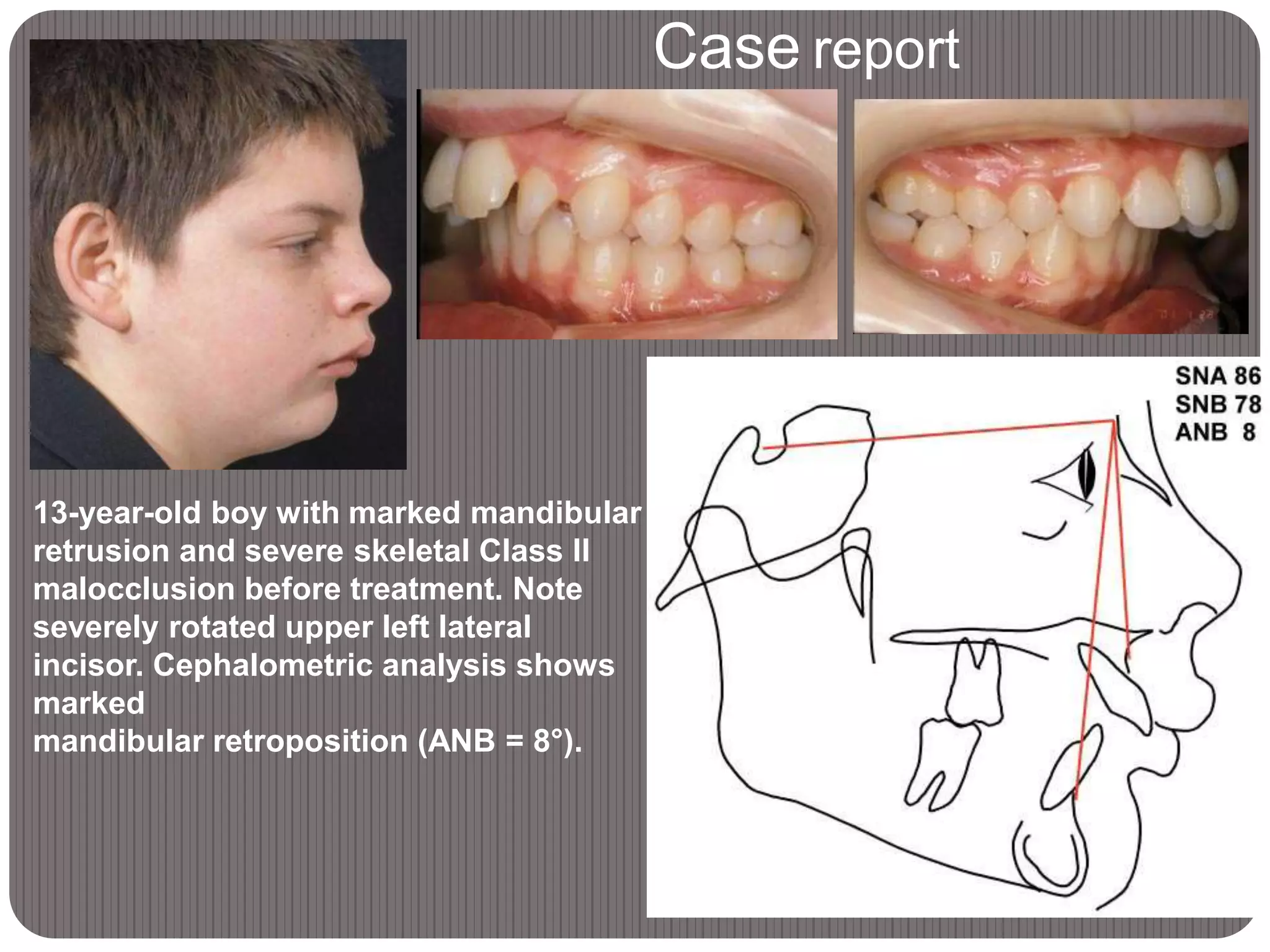
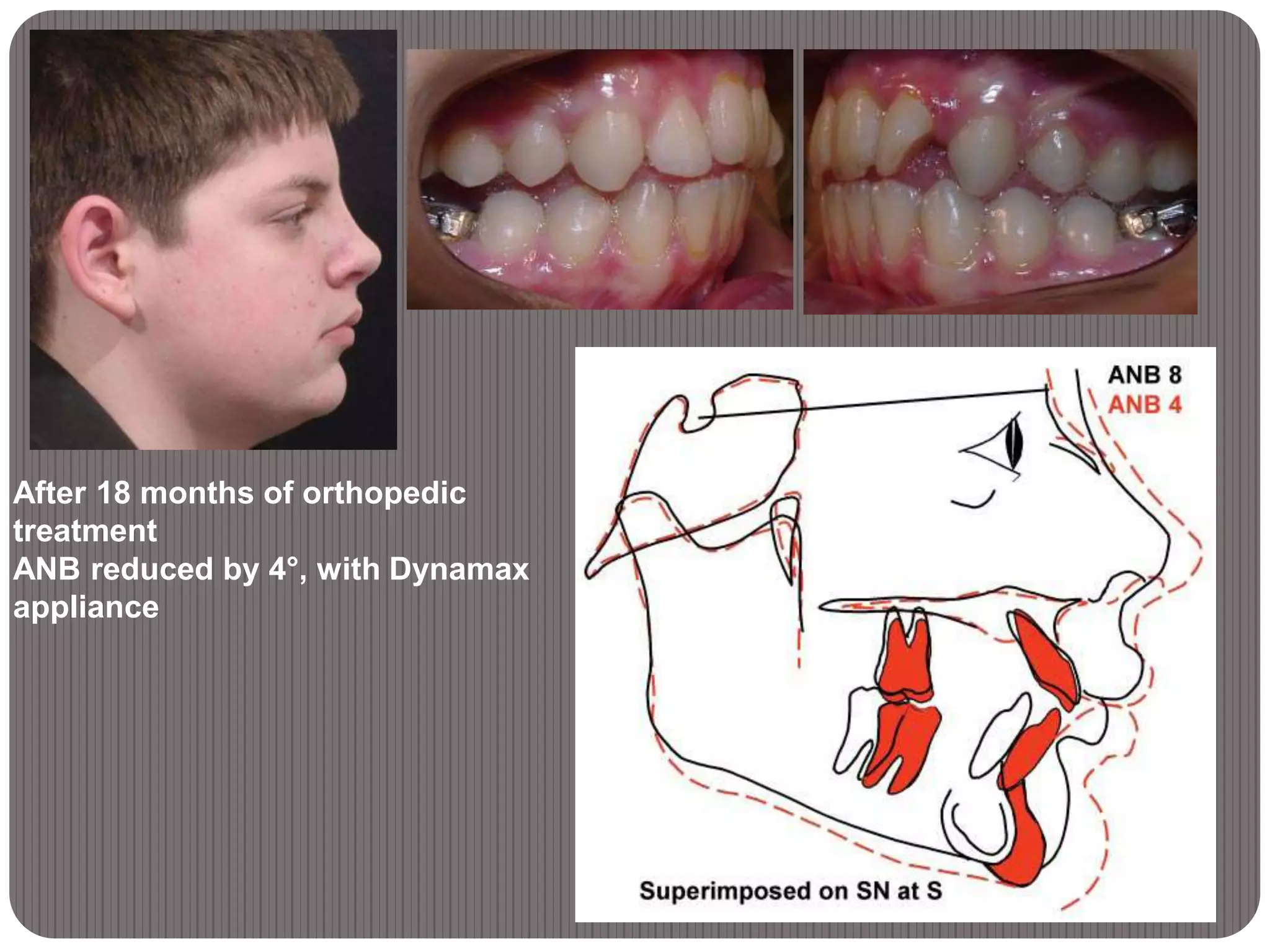
The Dynamax System is a new orthopedic appliance designed to treat skeletal Class II malocclusions. It has an upper removable component and a lower component that can be either removable or fixed. The appliance uses vertical springs on the upper component to engage "shoulders" on the lower component and advance the mandible into a protrusive position. It is constructed simply and can progressively advance the mandible in small increments to encourage growth. A case study showed that treatment with the Dynamax appliance for 18 months reduced a patient's ANB by 4 degrees. The Dynamax provides an efficient way to correct skeletal Class II malocclusions at any stage of dental development.