
More Related Content
What's hot
What's hot (20)
Similar to Texas chapter of the ACP annual meeting 2016 poster
Similar to Texas chapter of the ACP annual meeting 2016 poster (20)
Recently uploaded
Recently uploaded (20)
Texas chapter of the ACP annual meeting 2016 poster
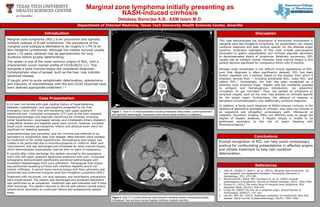
- 1. Marginal zone lymphoma initially presenting as NASH-induced cirrhosis Debdeep Banerjee A.B., ASM Islam M.D. Department of Internal Medicine, Texas Tech University Health Sciences Center, Amarillo Case Presentation Marginal zone lymphoma (MZL) is an uncommon and typically indolent subtype of B-cell lymphomas. The prevalence of the marginal zone subtype is estimated to be roughly 5-17% of all Non-Hodgkins Lymphomas. Although the median survival usually spans >10 years, patients may be asymptomatic for long durations before acutely deteriorating. The spleen is one of the most common origins of MZL, with a characteristic tumor marker profile of CD19/20/22 (+). This alongside a bone marrow biopsy are considered diagnostic. Extralymphatic sites of spread, such as the liver, may indicate advanced disease. If caught prior to acute symptomatic deterioration, splenectomy and induction of chemotherapy with the anti-CD20 rituximab have been deemed appropriate treatment.1-2 Introduction This case demonstrates the importance of extranodal involvement in marginal zone Non-Hodgkins Lymphoma. Its presentation can initially confound diagnosis and lead workup specific for the affected organ systems. Important highlights of this case include pancytopenia secondary to splenic sequestration and cirrhosis stigmata secondary to decompensated status of lymphoma. Relatively uncommon, MZL usually has an indolent course. However, bone marrow biopsy in this patient became significant for malignancy within only 8 months. Perhaps most remarkable is the difficult clinical appearance of MZL, such that diagnosis is often significantly delayed. MZL has been further classified into 3 entities, based on the location from which it originally derives from – including extranodal MZL, nodal MZL, and splenic MZL.3 Increasingly, the liver has been recognized as a distinctly local lymphoid organ. Hepatic cells are constantly exposed to antigens and hematogenous introduction, via splanchnic circulation, to gut microbes.4 Thus, the spread of lymphoma to lymphoid organs, such as the liver, may present as clinically specific for the target organ. Furthermore, the absence of regional or peripheral lymphadenopathy may additionally confound diagnosis. In addition, a faulty quick diagnosis of NASH-induced cirrhosis, in the absence of alternative etiologies of cirrhosis, may steer the clinician in an expensive and altogether unnecessary path. Ultrasound or magnetic resonance imaging (MRI) are effective tools to gauge the degree of hepatic steatosis, if hepatic biopsy is unable to be performed secondary to the risk of major bleeding with thrombocytopenia.5 Discussion Prompt recognition of MZL can help avoid unnecessary workup for confounding presentations in affected organs and initiate treatment to help halt condition deterioration. Conclusions References 1. Joshi M., Sheikh H., Abbi K., et. al. (2012). Marginal zone lymphoma: old, new, targeted, and epigenetic therapies. Therapeutic Advances in Hematology, 3(5), 275–290. 2. McDermott RS., Maher MM., Dunleavy K., et. al. (2002) Unusual presentations of lymphoma. Journal of Clinical Oncology, 20(7), 1943-1946. 3. Zinzani PL. (2012) The many faces of marginal zone lymphoma. ASH Education Book, 2012(1), 426-432. 4. Crispe IN. (2009) The liver as a lymphoid organ. Annual Review of Immunology 2009(27), 147-163. 5. Lee SS., Park SH. (2014). Radiologic evaluation of nonalcoholic fatty liver disease. World Journal of Gastroenterology, 20(23), 7392–7402. A 63-year-old female with past medical history of hyperlipidemia, diabetes, hypertension, and pancytopenia presented to her first emergency room (ER) visit with worsening right upper quadrant abdominal pain. Computed tomography (CT) scan at the time revealed hepatosplenomegaly and stigmata concerning for cirrhosis, including portal hypertension, esophageal varices, and intrahepatic biliary dilatation. Coagulation studies and hepatitis panel were normal; however, complete blood count revealed pancytopenia. History and physical exam were not significant for bleeding episodes. Gastroenterology was consulted, and her cirrhosis was believed to be secondary to nonalcoholic fatty liver disease. Beta-blockers were initiated for treatment of her portal hypertension. Percutaneous liver biopsy was unable to be performed due to thrombocytopenia of <60K/ml. After pain improvement, she was discharged and scheduled for bone marrow biopsy, which demonstrated hypercellular marrow with no signs of malignancy. 8 months after initial discharge, the patient returned to the emergency room with left upper quadrant abdominal distension with pain. Computed tomography demonstrated significantly worsened splenomegaly with consistent hepatomegaly from prior admission. Transjugular liver biopsy was performed revealing cirrhosis with interface hepatitis and B-cell marker infiltrates. A second bone marrow biopsy with flow cytometry was performed and confirmed marginal zone Non-Hodgkins Lymphoma (NHL). Treatment with rituximab, uric acid reducers, and neutropenic precautions were implemented. The patient was discharged and portacath placement was performed as an outpatient. Treatment was well-tolerated until 9 days after discharge. The patient returned to the ER with altered mental status, severe shock secondary to multiorgan failure and subsequently passed away. Figure 1. Axial CT on initial presentation revealing intrahepatic biliary dilation, portal hypertension, and significant splenomegaly. Subsequent bone marrow biopsy revealed no malignancy. Figure 2. Axial CT 8 months following initial admission revealing massive hepatosplenomegaly. Subsequent liver and bone marrow biopsies confirmed marginal zone NHL.