
More Related Content
What's hot
What's hot (20)
Similar to Systemic pathology cardiovascular system
Similar to Systemic pathology cardiovascular system (20)
More from TofiqueAhmed5
More from TofiqueAhmed5 (14)
Recently uploaded
Recently uploaded (20)
Systemic pathology cardiovascular system
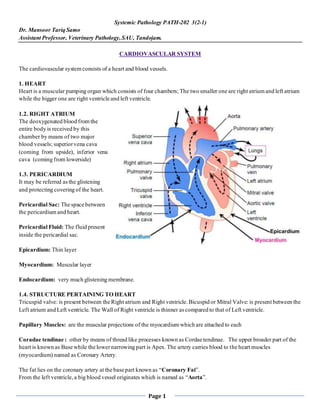
- 1. Page 1 Systemic Pathology PATH-202 3(2-1) Dr. Mansoor Tariq Samo Assistant Professor, Veterinary Pathology,SAU, Tandojam. CARDIOVASCULAR SYSTEM The cardiovascular system consists of a heart and blood vessels. 1. HEART Heart is a muscular pumping organ which consists of four chambers; The two smaller one are right atrium and left atrium while the bigger one are right ventricle and left ventricle. 1.2. RIGHT ATRIUM The deoxygenated blood from the entire body is received by this chamber by means of two major blood vessels; superiorvena cava (coming from upside), inferior vena cava (coming from lowerside) 1.3. PERICARDIUM It may be referred asthe glistening and protecting covering of the heart. Pericardial Sac: The space between the pericardium and heart. Pericardial Fluid: The fluid present inside the pericardial sac. Epicardium: Thin layer Myocardium: Muscular layer Endocardium: very much glistening membrane. 1.4. STRUCTURE PERTAINING TO HEART Tricuspid valve: is present between the Right atrium and Right ventricle.Bicuspid or Mitral Valve: is present between the Left atrium and Left ventricle. The Wall of Right ventricle is thinner ascompared to that of Left ventricle. Papillary Muscles: are the muscular projections of the myocardium which are attached to each Coradae tendinae : other by means of thread like processes known as Cordae tendinae. The upper broader part of the heart is known as Base while the lowernarrowing part is Apex.The artery carries blood to the heart muscles (myocardium) named as Coronary Artery. The fat lies on the coronary artery at the base part known as “Coronary Fat”. From the left ventricle,a big blood vessel originates which is named as “Aorta”.
- 2. Page 2 The small blood vessels coming to the left atrium are known as “Pulmonary Veins” while the vessel arising from the right ventricle is called “Pulmonary Artery”. THE HEART 1.4.1.1 GENERAL: The heart has an enormous capacity to deal with transient increases in workload, as long as adequate in tervals are provided for the recovery of nutritive and electrolyte levels. However, if the heart is forced to work against a sustained overload, it eventually becomes unable to deliver a normal output of blood. This leads to cardiac enlargement (dilatation and hypertrophy) which is the cardinal sign of heart disease. The onset of myocardial fatigue is characterized by slight acute dilatation of the heart which is due primarily to stretching of individual myocardial fibers subsequent to overfilling with blood during diastole. Eventually, the myocardium respondsto sustained overload by undergoing hypertrophy and chronic dilatation. Cardiac hypertrophy and dilatation are compensatory in nature and they usually occur together. However,in order for cardiac hypertrophy to develop,a healthy myocardium and adequate nutrition (blood supply) are required. If these factorsare lacking, dilatation in the absence of hypertrophy occurs. 1.4.1.2 HEART FAILURE Heart failure occurs when the myocardium is no longer able to compensate for increases in workload. "Congestive Heart Failure" is the clinical syndrome resulting from the inability of cardiac output to keep pace with venous return. It is characterized by pulmonary and/or generalized venous congestion and low cardiac output. Congestive heart failure is the final pathway of several important types of heart diseases. Subsequent to a failing heart, there is retention of sodium and water by the body (apparently from decreased renal blood flow and adrenal cortical mechanisms). This further distendsthe venous bed so that the heart cannot keep up with the amount of blood delivered. The clinical signs of congestive heart failure are the secondary effects of a failing circulation. Lesionsare most prominent and extensive in the lungs and liver. The componentsof the cardiac reserve are increased of rate of contraction and increased stroke volume; however, there are limits to the effectiveness of each. Increased stroke volume is the most effective of the two components. Lesions responsible for heat block are hemorrhages, infarction,and deposition of Ca, tumors, abscesses necrotic foci and fibrosis. There causes of heart block and the lesions must be close to and impinges the main parts of the condition system (The ventricular bundle or its right and left branches).The most crucial location of such lesionstherefore is in the dorsal aspects of the ventricular septum,where the ventricular bundle has its origin In cardiac failure (decompensation), many circulatory reflexes become active. The net effect is that of a coordinated sympathetic nervous system stimulation with reciprocal parasympathetic inhibition.The strong sympathetic stimulation increasesthe force of myocardial contractions and increases the tone in most of the blood vessels of the body. The normal cardiac output can be broadly defined as the output necessary to meet the needsof the organism at rest. The ability of the heart to respond to circulatory demandsover and above those of the animal at rest is referred to as the cardiac reserve.Any cardiac lesion which impairsthe efficiency of the heart reduces the cardiac reserve. Therefore, when the cardiac reserve is exhausted and the circulatory requirements of the animal at rest can no longer be met,"congestive heart failure" follows. Heart failure occurs in animals aswell, but the incidence is much lower. Heart failure can be broken down into two broad categories, acute heart failure and chronic (or congestive) heart failure. Congestive heart failure,also known as chronic heart failure,is the result of failure of the heart to maintain adequate circulation overa period of time. General causes of chronic heart failure include:
- 3. Page 3 • sustained systolic pressure overload, • sustained volume overload • loss of myocardial contractile capacity • interference with ventricular filling during diastole, The body makes many adjustments,or compensations, when faced with chronic heart failure. These adjustments to chronic heart failure can be divided into two main categories – peripheral and cardiac. Peripheral adjustments for insufficient cardiac output would include trying to maintain blood flow to vital organs, increasing the amount of red blood cells to help with oxygenation, and controlling the blood volume to decrease the load on the heart. Cardiac adjustments to heart failure are those compensations that allow the heart to respond to circulatory demands over and above those of the normal animal at rest. Congestive heart failure is often further divided into right-sided or left-sided heart failure. Failure on one side usually leads to failure on the other, so it doesn’t matter all that much. When one side of the heart fails.The ensuing sequence of events usually makes the opposite side fail as well. However, it is convenient to discuss the manifestations of left and right-sided heart failure separately. Remember, the manifestations of left and right heart failure apply to many of the diseases and conditions to be discussed later in this section. 1.4.1.3 LEFT-SIDED HEART FAILURE: The clinical signs of left heart failure are primarily pulmonary (lungs),and include dyspnea on exertion, cough, and orthopnea.Common causes of left heart failure include: • (1) myocarditis, • (2) degeneration of the myocardium, • (3) stenosis and insufficiency of the mitral and semilunar valves, and • (4) congenital heart diseases. Regardless of the cause, there is progressive dilatation of the left ventricle and atrium which may be followed by left ventricular and atrial hypertrophy. If the heart is unable to maintain a state of compensation, blood accumulates in the pulmonary veins and lung capillaries. Pulmonary (lung) congestion,edema, and induration ensue. The reduction in pulmonary vital capacity and impaired gaseous exchange result in hypoxic stimulation of the carotid sinus. Eventually, right heart failure develops subsequent to increased pulmonary resistance and increased pressure in the pulmonary artery (refer to the manifestations of right heart failure). It should be noted that coughing is usually the most distinctive and alarming feature of left heart failure in the dog. The productive cough is explained by the increased production of mucous, stimulated by severe lung congestion. 1.4.1.4 RIGHT-SIDED HEART FAILURE: Clinical signs of right heart failure are the manifestations of generalized venouscongestion,and include distention of the jugular and other superficial veins, liver and spleen enlargement, and an accumulation of fluid in serous cavities and in tissues (generalized edema).Common causes of right-heart failure include:
- 4. Page 4 • (1) left-sided heart failure, • (2) myocardial degeneration, • (3) myocarditis, • (4) factors that cause increased pulmonary resistance, • (5) hydropericardium, • (6) exudative pericarditis,and • (7) endocarditisand defective tricuspid and semilunar valves. Regardless of the causes, there is progressive dilatation of the right ventricle and atrium which may be followed by right ventricular and atrial hypertrophy.As the heart fails,blood accumulates in the vena cava leading to generalized venous congestion. Centrilobular congestion, degeneration, necrosis, and fibrosis of the liver ensue. The splenic red pulp becomes engorged, and there is generalized edema (ascites, etc.). Eventually, the effects of right heart failure are reflected in the left heart and lungs (if the animal lives long enough). Generalized edema is a prominent feature of right heart failure and there are some species differences in the location of the edematousfluid.In the horse and cow, a dependent subcutaneous edema is expected (subcutaneous edema is scant or absent in other species). In the dog, the predominant accumulation of fluid is in the peritoneal cavity (ascites); whereas in the cat, fluid is most commonly encountered in the thorax (hydrothorax). Remember, Cor pulmonale is the clinical term applied to right ventricular strain produced by diffuse pulmonary diseases (chronic emphysema, etc.). 1.4.1.5 HYPERTROPHYAND DILATATION OF THE HEART Remember, cardiac enlargement is the "cardinal sign" of heart disease. Myocardial hypertrophy is an increase in bulk of cardiac muscle due to an increase in size of component fibers. There are three descriptive types ofhypertrophy: SIMPLE HYPERTROPHY Is the term used when hypertrophy occurs in the absence of dilatation. ECCENTRIC HYPERTROPHY Is the term used when there is both hypertrophy and dilatation of the heart. Eccentric hypertrophy (volume overload hypertrophy). occursin response to chronic pressure-overloading caused by, systemic or pulmonary hypertension. Eccentric hypertrophy is characterized by increased ventricular chamber volume with normal ordecreased ventricular wall thickness. However, the total cardiac weight is increased due to a greater muscle mass surrounding the dilated chamber. CONCENTRICHYPERTROPHY Is the term used when hypertrophy results in a decrease in size of the heart chambers. Concentric hypertrophy (pressure overload hypertrophy). Occurs in response to chronic pressure-overloading caused by systemic or pulmonary hypertension. Concentric myocardial hypertrophy is characterized by increased ventricular wall thicknessand decreased ventricular chamber volume. Concentric hypertrophy must be accompanied by a compensatory increase in heart rate in order to maintain cardiac output. Hypertrophy affects the left heart more frequently than the right and the ventricles more frequently than the atria. Hypertrophy of the right heart makes the heart broader at the base; whereashypertrophy of the left heart increases the
- 5. Page 5 organ length. Bilateral hypertrophy results in a more rounded shape than normal. Grossly, increased thickness and a rubbery firmness are the best indices of cardiac hypertrophy. Cardiac dilatation may involve one or both chambers of the heart. Grossly, the dilated heart is globose shaped, the walls are soft, pliable, and thin. The endocardium is usually diffusely thickened and opaque. 1.6 PERICARDIUM OF THEHEART The pericardium is the fibro-serous sac which enclosesthe heart. The fibrousor outer layer is rather thin b ut strong and inelastic. The serous layer is an enclosed sac surrounded by the fibrouslayerand invaginated by the heart. It is smooth and glistening and normally contains a small amount of clear serousfluid.The parietal part of the serous layer lines t he fibrous layer,to which it is closely attached; whereas the visceral part of the serous layer covers the heart and partsof t he great vessels. This portion is referred to as the epicardium. Most diseases of the pericardium are secondary to disease processes in the heart, lungs, pleura,and other sites in the body. Usually, pericardial diseasesare detected clinically only when they cause an accumulation of fluid within the pericardial sac. 1.6.1 HYDROPERICARDIUM Hydropericardium refersto the accumulation of fluid (transudate) within the pericardial sac (remember, a small amount of clear fluid is found normally in the sac). Hydropericardium is caused by those factors responsible for generalized and/or local edema. Hydropericardium indicates the accumulation of serous fluid of non-inflammatory origin within the pericardial sac Hydropericardium is associated. 1. With conditions which increase the blood pressure of the coronary circulation. 2. In conditions in which there is decrease in the colloid osmotic pressure of the blood plasma. 3. With increased capillary permeability. Two good examples of condition which may raise the venous coronary pressure are stenosis and insufficiency of the right atrio-ventricular valve. The extra cardial lesions which may result in some venous disturbance are chronic pulmonary-emphysema and diffuses interstitial fibrosisof lung. As a result of any of these conditionsthe capillaries of the coronary circulation become dilated and the capillary blood pressure is raised.These conditions render the capillary wall more permeable to plasma protein and therefore the way foroedema to occur. Stomach worm infestation causes a decrease in the colloid osmotic pressure of the blood plasma which may result in hypropericardium. Remember, a small increase in pericardial fluid occursby transudation after death which is soon reddened by the products of postmortem hemolysis. 1.6.2 HEMOPERICARDIUM Hemopericardium refers to an accumulation of pure blood in the pericardial sac. The condition is uncommon in animals except in the following instances; • Following cardiac punctures. • Spontaneous rupture of the intrapericardial aorta of horses. • In uremic dogs with ulcerative atrial endocarditis.
- 6. Page 6 • Following rupture of the coronary artery. Remember, the term cardiac tamponade refersto compression of the heart subsequent to the accumulation of any fluid within the pericardial sac. The chief causes are trauma, spontaneous rupture (Degeneration)and dilatation (Aneurysm) and rupture of the coronary artery. 1.6.3 PNEUMOPERICARDIUM. Denotes air or gas in the pericardial sac.It may be result of a compound fracture and the penetration of a broken rib into the sac. It may also be due to gas forming organism in traumatic pericarditis. 1.6.4 PYOPERICARDIUM. Indicates the pus in the pericardial sac. It is the result of supportive or purulent inflammatory condition of the pericardium. It is commonly caused by micrococci and streptococci. 1.6.5 INFLAMMATIONOF THE PERICARDIUM(Pericarditis) Pericarditis refers to inflammation of both the parietal and visceral surfacesof the pericardium. A true pericarditis is nearly always infectious with an accumulation of exudate within the sac. Infectious agents usually reach the pericardium by extension from surrounding structures and/or by way of the blood stream (hematogenous route). The hematogenous route of infection is most common and the exudate tends to-be of the fibrinous or sero-fibrinous type.It should be noted that infection involving the pericardial (epicardial) surface seldom showsan appreciable spread into the underlying myocardium. 1.6.5.1 FIBRINOUS PERICARDITIS is a characterized by an accumulation of fibrin within the pericardial sac. In many cases the exudate coagulates, forming a thin fibrinouscovering over the pericardial surfaces. Such a form is known as fibrinous pericarditis. Where the exudation is profuse and much fibrin is formed, the rubbing together of the fibrin-covered surfaces causes the heart to assume shaggy or so called bread and butter appearance. Grossly,the fluid is grayish to yellow, and flecks of blood may be present. In cattle, it is commonly a part of blackleg, pasteurellosis, contagious bovine pleuropneumonia,sporatic bovine encephalomyelitis, and some forms of neonatal coliform infections. In swine, fibrinous pericarditis is frequently associated with Glasser's disease, pasteurellosis, and salmonellosis. In the horse, streptococci are usually present. 1.6.5.2 PURULENT PERICARDITIS is characterized by the accumulation of pusin the pericardial sac (due to pyogenic bacteria) and may be associated with septicaemia or pyaemia. It occurs most commonly as a result of traumatic perforation by a foreign body originating from the reticulum (traumatic pericarditis). Also, in traumatic pericarditis the exudate may be fibrinous or fibrino-purulent in nature. Pus within the pericardial sac may appearas a thin cloudy exudate, as frank creamy exudate, or as a mixture of purulent exudate and masses of pus.The accumulation of pusin the sac places tension on the pericardium which may be reflected in pooling of venous blood (congestive heart failure). In both fibrinous and purulent pericarditis,healing is usually by organization.
- 7. Page 7 Ultimately, the organizing fibrous connective tissue joins the two surfaces of the serous pericardium resulting in an adhesive pericarditis. Thus, considerable pressure is exerted, and the heart muscles become more or less rigid (constrictive pericarditis). This pressure on the myocardium and large vesselscausescompensatory ventricular dilatation and hypertrophy.Subsequently, generalized venous congestion occursand death may ensue from "congestive heart failure." 1.6.5.3 TRAUMATICPERICARDITIS This condition occurs in cattle as a result of traumatic perforation of the pericardium by a foreign body originating in the reticulum (traumatic reticulitis). In cattle,this form arises from the swallowing of a foreign body such as nail, needle or a piece of wire.This become lodged in the reticulum and on account of the muscular contractions, is some times driven in to the mucous membrane. The foreign body may then be forced through the reticulum wall into and through the diaphragm.The entrance of bacteria along with the foreign body gives rise to inflammation and ulceration, producing a supportive tract.Adhesions are formed between the reticulum and diaphragm. The latter is usually pierced opposite the apex of the heart, and the continued forward movement of the foreign body some -times leads top perforation of the pericardium and occasionally the heart. (as well as the myocardium and endocardium) resulting in an exudative pericarditis). At the end it may cause, lesions in the pleura and lungs and even in the liver,spleen and peritoneum. The penetration of the pericardium by foreign body sets up pericarditis but the type of inflammation which results depends on the nature of the organism which accompanies the foreign body. It is generally purulent but it may be fibrinous, sero-fibrinous or hemorrhagic. The heart itself is commonly hypertrophied due to the hampering of its action by exudatesand adhesions. 1.6.5.4 SEROUS ATROPHY OF PERICARDIAL FAT In any cachexia and/or debilitating condition,there is progressive mobilization of depot fat, including that beneath the epicardium. As normal lipid vacuolesare reduced in size,they are replaced by a proteinaceous fluid; subsequently,normal fat is converted to grayish-brown gelatinous masses. 1.7 ENDOCARDIUM OF THE HEART The endocardium linesthe cavities of the heart, and is continuous with the intima of vessels which enter and leave the organ. Its free surface is smooth and glistening and is formed by a layer of endothelial cells. This endothelial layer rest o n a thin layer of fibroelastic tissue which is connected to the myocardium by subendothelial elastic tissue containing nerves and vessels. 1.7.1 INFLAMMATIONOF THE ENDOCARDIUM Endocarditis refersto inflammation of the endocardium which may be valvular ormural. In domestic animals, valvular endocarditis occurs more frequently than mural. Endocarditis is usually caused by bacterial agents, but occasionally parasites and mycotic agents may serve as causative factors. A large number of bacteria are capable of causing endocarditis; however, the manner by which these bacter ia localize on a valve is not clear.Apparently, endocarditis occurs subsequent to a substained or recurrent bacteremia. In the dog and horse, streptococci and staphylococci are most commonly isolated from valvular lesions: whereas Corynebacterium pyogenes is most frequently recovered in cattle. The location of endocarditis varies with the animal species involved. In cattle,lesions are most common in the right heart; whereas in the horse. dog, and pig, endocarditis occurs most frequently in the left heart. In cattle, the tricuspid valve is
- 8. Page 8 most commonly affected followed by the mitral, pulmonary, and aortic valve. In the horse, the aortic valve is most frequently involved, followed by the mitral and finally the pulmonary valve. In the pig and dog, lesions are most commonly observed in the mitral valve, followed by the aortic,tricuspid, and the pulmonary valve. Acute ulcerative mural endocarditis is commonly encountered in dogs suffering from acute renal insufficiency (uremia). The lesions (ulcers and thrombi) occur primarily in the left atrium, but may be found in the left ventricle and large elastic arteries. Experimentally, lesionsoccurmore commonly in dogs fed diets high in fat prior to the onset of renal failure. Also, ulcerative mural endocarditis occurs frequently in the left atrium of calves with blackleg. Regardless of the cause, thrombi are formed in those areas where the endothelium is damaged (valvular or mural). The terms "vegetative" or "cauliflower" are commonly used to describe the gross appearance of these thrombi. The surfaces of the thrombi are friable and embolism may occur. Organization proceeds from the base by the usual process of granulation. Remember, valvular thrombi are almost always serious since they tend to obstruct the normal flow of blood, prevent perfect closure of the valves, and/or result in embolism. 1.7.2 CALCIFICATION OF THEENDOCARDIUM Calcification of the elastic fibers of the endocardium is encountered in dogs, cattle, sheep, and horses. In dogs, endocardial calcification occurs most commonly in those which have recovered from acute ulcerative endocarditis of renal insufficiency.It occurs in calvesand lambs with vitamin E and selenium deficiency (white muscle disease), and in older cattle with hypomagnesemia. Also, endocardial calcification may be associated with any debilitating disease. 1.8 MYOCARDIUMOF THE HEART 1.8.1 INFLAMMATIONOF THE MYOCARDIUM Myocarditis refers to inflammation of the myocardium, which is usually secondary to a wide variety of systemic diseases. The causative agents may reach the myocardium by extension or by the hematogenous route. The lesions are usually focal and may be overlooked on causal gross inspection. 1.8.1.1 SUPPURATIVEMYOCARDITIS Is associated with the presence of pyogenic organisms, and abscessformation is common. The inflammation is usually localized and is characterized by the formation of abscesses. The bacteria reach the myocardium by way of the blood stream or extension from adjacent organs. As a result, local suppurative myocarditis is associated with septicemia or bacteremia when the organismsare carried to the heart from suppurative processesin other organs. Septic emboli may lodge in a coronary artery and produce an abscess.The myocardium may also be involved in suppurative inflammation by extension of process from a near by inflamed organ or part e.g. from the pericardium, endocardium, plura lungs,bronchial or mediastional lymph glands. 1.8.1.2 NON-SUPPURATIVE MYOCARDITIS Is associated with various toxemias. The irritant may be mineral, poison or toxin from bacterial or parasitic infections or necrotic tissue as occurs in coagulative necrosis. 1.8.2 DEGENERATIVE AND RELATEDCHANGES OF THE MYOCARDIUM
- 9. Page 9 Cardiac muscle is subject to the same type of degenerative changes as skeletal muscle. However, there is a greater tendency for heart muscle to undergo degenerative changesas a response to non-specific causes. HYALINE CHANGES (and necrosis) of the myocardium occursas a part of "white muscle disease syndrome" and gossypol poisoning. Calcification of the myocardium is usually dystrophic in type, and it occurs whenever there are dead or dying myocytes. In organomercurial poisoning of cattle, calcium salts are selectively deposited in the purkinje network. 1.8.3 NECROSIS ANDISCHEMIA OF THE MYOCARDIUM Myocardial infarction precipitated by arteriosclerosis of the coronary artery is a burden of aging humans, but is rare in domesticated animals.In animals however,acute obstruction of the coronary arteries due to emboli occurs with some frequency,with the development of infarction.If the coronary obstruction is chronic, the end result is diffuse scarring of the myocardium and markedly altered function. Coagulative necrosis of the myocardium is a lesion commonly associated with vitamin E and selenium deficiency (white muscle disease) in lambs,calves, and pigs. 1.8.4 HEMORRHAGES OF THE HEART AND ITS MEMBRANES Petechial, ecchymotic,and larger hemorrhages occur beneath the epicardium and endocardium asagonal changes. Agonal hemorrhages are due to anoxia and rupture of small vessels that occurduring the process of dying. Also,subendocardial and subepicardial hemorrhages are commonly associated with septicemias, bacteremias, toxemias, and hypoxic conditions. VASCULITIS is defined as an inflammation of vessels characterized by presence of inflammatory cells within and around vessel walls. Lesionscan be more specifically designated asarteritis (arteries), phlebitis (veins),or omphalophlebitis (umbilical veins). Vasculitis is commonly associated with septicemic, viremic, and toxemic diseases. Endothelial cell damage is a primary factor in the pathogenesisof many diseasesincluding: canine herpes, infectious canine hepatitis, swine fever, heartwater, African horse sickness,epizootic hemorrhagic disease, bluetongue and endotoxemia. 1.10 ARTERIES 1.10.1 Inflammation of Arteries (Arteritis) Arteritis is characterized by the presence of inflammatory exudate (neutrophils, etc.) within the layersof the vessel wall. A non-specific type of arteritis is a component of all acute inflammatory lesions. The inflammatory reaction occurs in arteries which pass through inflamed areas,or which contain infected thrombi oremboli. It is usually the smaller arteries that are involved and the arteritis is, therefore, of little consequence except in cases of thrombolic infarction or embolism. In general, non-specific arteritis is secondary to and correlates directly with the inciting cause. Specific types of arteritis occur in a wide variety of systemic infectious diseases.Damage may be due to direct effect of a microbial agent or its toxin on any component of the vascular wall. In the horse arteritis commonly occurs subsequent to invasion of the anterior mesenteric artery by immature Strongylus vulgaris. Also, arteritis is an important lesion in Newcastle disease of birds, equine viral arteritis, malignant catarrhal fever, renal insufficiency in dogs, dirofilariasis, etc. Arteritis subsequent to immunologici injury occurs when munecomplexes (antigen/antibody/complement) attach to vascular endothelium. Initially, antigens localize in vascular walls and subsequently complex with circulating precipitating antibodies. The antigen/antibody complexes attract complement. The arteritis is caused by neutrophils for which the complement containing complexes are chemotactic (neutrophils are attacked by terminal complement fragments). Immunologic arteritis occursin the Arthus reaction,acute serum sickness. Aleutian disease,and in cases of
- 10. Page 10 glomurulo-nephritis. The Arthus reaction is the classical experimental model of immune complex disease and the basic lesion is an intense arteritis. 1.11 SOME SPECIFIC DISEASES AND CONDITIONS CHARACTERIZEDBY ARTERITIS 1.11.1 EQUINE VIRAL ARTERITIS 1.11.2 ARTERITIS OF RENAL INSUFFICIENCYOF DOGS 1.11.3 DIROFILARIASIS 1.12 Non inflammatory Lesionsof Arteries 1.12.1 CALCIFICATION: Arterial calcification occursfrequently in animals as a dystrophic or metastatic process. Calcium salts may be deposited in the intima or media. Calcification of the media is commonly associated with chronic renal insufficiency in dogs, vitamin D toxicosis, and a variety of debilitating diseases of cattle. 1.12.2 ANEURYSM OF ARTERIES An aneurysm is a pathological, more-or-less circumscribed, dilatation of an artery (or chamber of the heart). The arterial wall is composed of stretched intima and adventitia with only remnants of media. There is a tendency for aneurysms to enlarge progressively and to ultimately rupture. A false aneurysm is a blood-containing cavity that communicateswith the arterial lumen. The wall is formed from surrounding tissues. A dissecting aneurysm is characterized by the presence of blood between the layersof the arterial wall (usually in the media). The blood current gains access to a defect in the media and the resulting blood pressure forcesthe blood for some distance between the layers. ANEURYSM: It is a local dilatation of an artery Aneurysm of an artery,when of recent formation,has a wall consisting of the three arterial layers.In older lesions,the normal structure of the wall disappears and being replaced by granulation tissue of which may contain cerium the deposits. An aneurysm is a localized dilatation of an artery. Dilatations of the veins are called varicosities (singular varicose) rather than aneurysms. A true aneurysm results from formation of a sac by the arterial all three walls layer. It is most often associated with atherosclerosis. A false aneurysm usually is caused by trauma. In this case, the wall of the blood vessel is ruptured and blood escapes into surrounding tissues and formsa clot (hematoma). CLASSIFICATION. 1. A fusiform aneurysm; is spindle shaped.Entire circumstance dilates and the aneurysm is spindle shaped. 2. A saccular aneurysm; is one-sided dilatation where only part of the circumference is involved. 3. A dissecting aneurysm; as the name suggests occurswhen the blood accumulated in between the coat of the artery wall following a damaged intima. 4. Millary aneurysm; are very small aneurysm which are found in the cerebral arteries. 5. A cricoid aneurysm; which is sometimesfound in subcutaneous tissues, consists of a mass of dilated and tortuous arteries which formsa pulsating swelling. It is congenital. 6. A traumatic aneurysm is a false aneurysm which follows rupture of an artery wall, the blood accumulating in the connective tissue. CAUSES. An aneurysm results from the pressure of blood on the wall of an artery, which has been weakened through one cause or another. Often there are no symptoms,but a ruptured aneurysm can lead to death. Rarely but can been seen in older animals. The following are the chief causesin animals.
- 11. Page 11 1. Parasites, e.g. strangles vulgaris larvae in the anterior mesenteric artery of the horse. The aneurysm may become as much as six inches in diameter when involving the truck of the anterior mesenteric artery. 2. Trauma, Disease of the artery wall, e.g. atheroma,Embolism. SEQUALAE. 1. Aneurysm may rupture and cause death. 2. They may cause pressure atrophy of the surrounding tissue and, if important structures are involved death may follow. 3. The contentsof the aneurysm may give rise to embolism. 4. Thrombosis and complete stoppage of the circulation through the vessel may occur. 5. Parasitic aneurysms of the mesenteric artery of the horse may cause colic. 1.12.3 HYPERTROPHYOF ARTERIES Hypertrophy of arteries may affect one orall componentsof the vascularwall. It occurs in response to the need to carry an extra load. Medial hypertrophy of the pulmonary arteries occurs commonly in the lungs of cats. The condition is characterized by marked hypertrophy of the muscular media so that the lumen is reduced to rather small slits. There are no apparent clinical signs and the cause is unclear. 1.12.4 ARTERIOSCLEROSIS : is an umbrella term for several types of changes that cause hardening of arteries. Arteriosclerosis without lipid deposition can occur due to increased connective tissue, vascular mineralization (Johne’s disease), or hyaline degeneration (Coronary arteries of old dogs). Ateriosclerosis with lipid deposition, also known as atherosclerosis,is common in humansbut infrequent in animals. Arteriosclerosis literally means hardening of the arteries. It includes those degenerative changes characterized by induration (fibrous thickening), lossof elasticity, and narrowing of the lumen. Usually arteriosclerotic lesionsdevelop as multiple or focal sclerotic changes superimposed upon a generalized,age-related increase in connective tissue elements of the vessel wall. The "hallmark" of arteriosclerosis is the fibrous plaque which appears as a white, firm, glistening elevation on the luminal surface of arteries. The well-developed fibrous plaque consists largely of "modified" smooth muscle cells (myocytes) surrounded by increased amounts of extracellular matrix. Subclassifications within the broad category of arteriosclerosisare atherosclerosis,medial sclerosis, and arteriolosclerosis. Atherosclerosis is characterized by the accumulation of lipid in larger arteries in the form of elevated,lipid-filled plaques called atheromas. The atheroma beginsas an intimal lesion which progressively extends into and affects the media. In animals, atherosclerosis occurs primarily in the aorta and small muscular arteries. In the dog, severe systemic atherosclerosis is associated with advanced age, obesity, and hyperlipoproteinemia . The majority of these dogs have hyperthyroidism which leadsto hypercholesterolemia and, indirectly,to atherosclerosis. In aged humans, atherosclerosisis an extremely common lesion and disease. The aorta, coronary, iliac, and cerebral arteries are most often affected.Because atherosclerotic lesionscan occlude blood vessels, serious consequences such as myocardial infarction and stroke may occur. ATHEROMA
- 12. Page 12 It is a localized or patchy condition of in timed thickening of arterial wall (due to deposition of lipids and formation of fibrous tissue) which is more often found affecting the aorta, particularly at the arch or the point of exit of other blood vessels. The lesions may also involve the coronary and cerebral arteries and sometimesthe endocardium. CAUSES: Little is known regarding the causation of the condition and have a toxic origin orit may followdietetic errors. NAKED EYE APPEARANCES. In the larger vessels, such as the aorta,the lesion is in the form of hard,well-defined, whitish or yellowish spots which project in to the lumen of the vessel. The colour is due to the presence of fatty changes in the deeper layers of the intima, and the hardnessfollows the deposition of lime salts.The smaller vessels are characterically tortuous. MICROSCOPIC APPEARANCES. The changes in atheroma are confined to the intima,and the features of thiscondition,both proliferative and degenerative changes are present. The superficial layer of the intima presents an increased amount of connective tissue, and the deeper layer, fatty degeneration is prominent. SEQUALAE. 1. Weakening of the arterial wall may lead to dilatation and the formation of the aneurysm. 2. The occurrence of thrombosis or the narrowing of the lumen may lead to nutritional changes,e.g. disease of the coronary arteries causes atrophy and fibrosis of the heart. 3. The disease may extend to the endocardium. 4. Ulceration may occur and embolism and infarction result. 1.12 VEINS 1.12.1 Inflammation of Veins (Phlebitis) Phlebitis is the inflammation of veins characterized by presence of inflammatory exudate, thickening of the wall and dilation of the lumen. The condition is less common than arteritis. Some time occurs with thrombophelibitis and Omphalophlebitis. Omphalophlebitis in which the umbilical veins, particularly in farm animals, become infected and inflamed after birth. Acute phlebitis occurs in "navel infection" (omphalophlebitis) of calves, lambs and foals. Some parasitessuch as Schistosoma sp (blood fluke trematode) cause parasitic phlebitis. ACUTE PHLEBITIS: Is invariable result of bacterial infection and is always associated with thrombosis. CAUSES. 1. Blood infection. The organisms present in the blood, setup inflammation of the endothelial lining and thrombosis results. 2. Extension from neighboring inflamed tissue as in the utrines veins from septic metritis. 3. A phlebitis of the jugular vein (vine section)may arise as the result of improper intravenous injection or faulty techniques. 4. Omphalophlebitis-phlebitis occurs in young animalsbefore the umbilicus has healed. MACROSCOPICALLY.
- 13. Page 13 The wall of the umbilical vein is thickened, the lumen dilated and contains thick necrotic material, after removal of which the inner surface of the vessel appears rough and redden. MICROSCOPICALLY. There is pronounced leococytic infiltration of the wall but gradually becomes less in number from within out. Other pathological conditions which may involve veins are asfollows. 1. Spontaneous rupture, most frequently in the posteriorvena cava. 2. Thrombi formation, seen in the mammary, portal and uterin veins. 3. Parasitic obstruction. SEQUELAE. 1. Resolution may occur. 2. The thrombus may become organized and obliteratesthe lumen of the vein. 3. In suppurative affection, septic emboli may cause pyaemia. 4. The thrombus may classify and form a phelebolith. 5. Embolism of the pulmonary artery. THE LYMPHATIC SYSTEM is a network of organs (i.e tonsils, spleen and thymus), cells (lymphocytes), ducts (lymph vessels), and glands (lymph nodes) can be found throughout the body. Lymph travelsthrough the body along lymphatic vessels and collects fats, bacteria, and other waste products from cells and tissues. The lymph nodes then filter these harmful materials out of the fluid and produce more white blood cells to fight off the infection. PATHOLOGICALCONDITION OF LYMPHATIC SYSTEM Lymphangitis is an inflammation of the lymphatic system, which is a major component of the immune system. Lymphadenitis Inflammation of lymph glands. Lymphatic system problems can include infections, blockage,and cancer. Lymphoid leukaemias and lymphomas are nowconsidered to be tumours, “Leukaemia" when tumour in the blood or marrowand “Lymphoma" when tumour in lymphatic tissue. And togetherthey called “Lymphoid malignancy" LYMPHADENITIS. Inflammation of lymphatic gland. Acute lymphadenitis is found in many cases of the acute septicaemic diseases especially in the early stages and in the nodes draining an organ or part of the body undergoing acute inflammation. Bronchial lymph glandsare unchanged and inflamed in pneumonia, supra mammary glands depends simply to mastitis, pharange at swell in rhinitis or infected with. It is frequent in acute septicaemia such as anthrax, pasteurellosis. In the mesenteric nodes it is one of the lesions of suckling calves,lambs and kids. MACROSCOPICALLY. The lymph nodes are enlarged and soft, the cut surface is moist,bulgesand is reddened. MICROSCOPICALLY. There are hyperaema,oedema and haemorrhage (erythrocytes in the lymph sinuses),In the parenchyma of the gland the lymphoid hyperplasia may produce atrophy of the germinal centers. CHRONIC LYMPHADENITIS.
- 14. Page 14 Chronic lymphadenitis occurs in the mesenteric lymph nodes of cattle with paratuberculosis. Bovine tuberculosis is a chronic inflammation usually characterized by caseous necrosis and calcification.The enlarged, firm, grey nodes contain cheesy yellowarea which are often gritty when cut. In glanders, actinobacillosis and actinomycosis a chronic suppurative lymphadenitis occurs. In any of these diseases the nodes are enlarged usually and contain thick walled abscess cavities. LYMPHANGITIS INFLAMMATIONOF THE LYMPHATIC VESSELS. Acute sero fibrinous lymphangitis occurs in the lungs in the course of inflammatory diseases (catarrhal pneumonia of dogs and horses)characterized by peribronchitis and peribronchiolitis. Acute suppurative lympangitis arises in connection with suppurative processes in the area drained by the affected lymph vessels. Chronic suppurative lymphangitis is an important lesion in glanders,epizootic and ulcerative lymphangitis of horses. Lymphangitis occurswhen viruses and bacteria invade the vessels of the lymphatic system, typically through an infected cut or wound. Lymphangitis occurs when bacteria or virusesenter the lymphatic channels. They may enter through a cut or wound, orby an existing infection. Bronchial lymph glands are involved and inflamed in pneumonia cases. In mastitis, enlarged supramammary, iliac and lumbar lymph nodes. Also Mycobacterium paratuberculosis & Brucella abortus infection. Pharynges are involved due to tonsils swelling in rhinitis or in infection. LYMPHEDEMA: If lymphatic system not working properly, fluid builds in body tissues and causes swelling, called Lymphedema. Lymph edema classified into primary and secondary • Primary lymph edema is usually congenital and hereditary due to anomalous development of the lymphatic system. • Secondary lymph edema occurs because of obstruction of previous normal lymphatic duct due to infection, inflammation, tumour,or injury. Lymph edema is because of the predispose affected area,usually limb, to secondary bacterial infection and poor wound healing. LYMPHATIC FILARIASIS is caused by the worms Wuchereria bancrofti, Brugia malayi,and Brugia timori. These worms occupy the lymphatic system, including the lymph nodes; in chronic cases, these worms lead to the syndrome of ELEPHANTIASIS.These are transmitted by mosquitoes and their life cycles are start.Infective larvae enter peripheral lymphatics, migrate to nearest lymph nodes and develop 2 weeksbefore migrating to nearest lymph nodes and mature their and produce gramalomatous lymphangitis and lymphadenitis and cause lymphoedema and elephantiasis. CHYLOTHORAX: characterized by the accumulation of chyle within the thoracic cavity due to leakage orrupture of the thoracic duct. Infrequently seen in dogs and cats.Chyle hasa characteristic milky color contains small molecules of fat after digestion. the fatty component of the meal is further broken down into small molecules termed chylomicrons. The intestinal lymphatic system that travels to a structure called the cisterna chyli (CC), which is locate in the front portion of the abdomen, near the kidneys, absorbs these small molecules. The CC is a lymphatic reservoir that receives chyle from the intestine but also receives lymphatic fluid from the rest of the abdomen and pelvic limbs. The thoracic duct (TD) is the extension of the CC into the chest, which carries chyle into the thoracic cavity and eventually emptiesits contents into the cranial vena cava (CrVC) close to the heart. In pets affected with chylothorax there is an abnormality in the TD that causesit to leak chyle into the thoracic cavity. These pets have difficulty breathing as the chyle that buildsup in the chest prevents their lungs from fully inflating with air. The lymphatic fluid that is also a main component of chyle contains protein, white blood cells, and vitamins.The lossof large amounts of chyle into the thorax can weaken your pet’s immune system and create severe metabolic disorders.Chyle is also an irritant and chronic
- 15. Page 15 exposure to the lining of the lungs (pleura) and heart (pericardium) can lead to inflammation of those surfaces with further deleteriousconsequences. PATHOLOGICALVARIATION OF REDCORPUSCLES. A. VARIATION IN NUMBER. 1. Polycythemia. Increase in number as seen in diarrhea and excessive perspiration. 2 Olygocythaemia. Decrease in number. The condition is present in anaemia or piroplosmosis. B. ANISOCYTOSIS. Variation in the size of erythrocytes seen in anaemia. Cells smaller than average red cell are called microcytesand those larger than average are called as megalocytes.Still larger are called as gigantocytes. C. POIKILOCYTOSIS. Variation in shape is seen in anaemia. D. NUCLEATED FORMS ORERYTHROBLASTS. Erythroblasts are seen in severe forms of anaemia . They are seen in bone-tumour and myeloid leukaemia. If the cell are larger than normal they are called megaloblast and if smaller microblasts. Mucleated SRBCS of normal size are called normoblasts. E. VARIATION IN STAINING REACTION. 1. Plychromasia or Basaphilia: Cells having bluish tint. 2. Punctate basophilia.Where the cells are studied with purple stained granules. Seen in chronic lead poisoning and anaemia of toxic origin. 3. Reticulated cells. These are young cells which have recently lost theirnuclei and in which a definite reticulum is apparent. PATHOLOGICALVARIATION OF LEUCOCYTES. A. Variation in numbers. Leucocytosis: Increase in number of leucocytesgenerally neutrophils seen in suppurative conditions and in malignant growing conditions. Lymphocytosis: Increase in number of lymphocytes, this is seen in chronic wasting diseases, rickets and following the injection of tuberculin. Eosinophilia: Increased number of eosinophils. It occursin chronic skin disease, some formsof sensitizations. Leucopenia: Decreased number of leucocytes. Seen in certain virus infections, anemia, starvation and malnutrition. B. VARIATION IN TYPE. 1. Myeloblast: This is the precursor of all granular leucocytes. Presence in circulation indicates some interference with the function of formative bone-marrow. 2. Myelocytes: seen in myloid leukaemia and rarely in acute cases of “Anaemia”. 3. Lymphoblast: Seen as precursorof lymphocyte and is seen in circulation in lymphatic leukaemia.
- 16. Page 16 ANAEMIA: Is a deficiency of erythrocytes or of haemoglobin or of both.While the most frequent forms of anaemia are characterized by the deficiency of erythrocytes but there can be an anaemia characterized by too little haemoglobin in each cell, the numberof cells being normal. Since in anaemia, the erythrocytes may have the normal size or may be enlarged or diminished in size. In case the size is normal it is temed as normocytic and when the red cells are smaller in size it is designated as microcytic anaemia. The anaemia is called ashypochromic if the quantity of haemoglobin in each cell is lese than normal and colour is pale, the oxygen capacity is reduced even of the red cell count is normal.A normochrome cell contains a saturated solution of haemoglobin from the stand point of causation,the anaemia may be classified as follows. TYPES OF ANAEMIA. 1. Haemorrhagic anaemia. 2. Haemolytic anaemia. 3. Aplastic anaemia. 4. Deficiency anaemia. 1. HAEMORRHAGIC ANAEMIA. Results from severe haemorrhage.Chronic haemorrhagic anaemia arisesfrom continued loss of blood or a series of small haemorrhages e.g. Parasites Haemonchus contortus of sheep and Stranglesof the horse Poikylocytosts distinet in this form of anaemia. 2. HAEMOLYTIC ANAEMIA. Results from excessive distruction of the circulating erythrocytes,occurring within the blood stream. The blood picture shows nucleated red cells, and reticulocytes. The causesare as under. 1. Piroplasmosis. 2. Anaplasmosis. 3. Virus of equine infections anaemia. 4. Trypanosomiasis, acute bacterial infectionsincluding those due to Cl. Haemolyticum and Cl. Velchii.Certain Aemicals, poisions have a similar effectsincluding. Pot and sod chlorides,lead usually is a chronic poioning. 3. DIFICIENCY ANAEMIA. (a) Due to defective absorption and assimilation of factors necessary for haemoglobin formation chiefly iron and other substancessuch as Cu, Co, manganes etc. (b) Due to defective production or assimilation of anti-anaemic factor. The formation of red corpusclesin the bone marrowdepends on several specific and nonspecific factors. The specific factorsare iron and erythrocyte maturing or antianaemic factorpresent in liver and stomach.It is said that most animals secrete in normal gastric juice an intrinsic enzyme factorsand this interacts with extrinsic substances present in certain food and formsas haemopoietic or antianaemic factor which is stored in the liver from here this factor conveyed when required, to the bone-marrow, where it is necessary for the maturation of the red blood-corpuseles before they are released into the blood stream. Aplastic anaemia, in this form of anaemia the haemopoitic tissue of the bone marrow are infected in such a away that their ability to produce erythrocytes is impaired or destroyed.The causes of this type of anaemia are either toxic radiation or toxic substance brought to the marrow cells in the circulating blood.Irradiation whether rays, X. Rays,radium or radio active isotopes,is highly destructive of the hemopoietic tissue and this action is the chief reason that any butvery small dosage are lethal. SIGNIFICIANCES AND EFFECTS OF ANAEMIA. Anoxia of the tissuesis the most important product of anaemia that lead to fatty degeneration of the myocardium and other susceptible organs and even Necrosis supervene.
- 17. Page 17 In haemolytic anaemia the spleen contains Phagocytised haemosidrium. When oedema accompanies anaemia it is due to increased permeability. CHANGES IN ANAEMIA. The red carpusels which may be reduced in number are pale in colour due to deficiency of haemoglobin, Anisocytosis like Leucocytosis,polychromia and nucleated from are sometimes seen. The mucus membranes r eveal haemorrhagesand tissues are often oedematous. The organs are pale but the lymphatic glands and lymoid tissues show no changes. When there is great cell destruction haemosiderous becomes evident in some organs. PERNICIOUS ANAEMIA. This anaemia in man appears to result from the absence of the anti-anaemic factor. Neither thiscondition has been recognized in animal nor it has been produced experimentally but it is possible that absence of this factor may play a part in some anaemia in animals. LEUKAEMIA. Leukaemia is a disease of the leucocyte forming tissue in which hyperplastic changes occur, these being associated with an increased in the number of leucocytes, many of them immature in the circulation. The causes of the condition is unknown but it is regarded by some as form of neoplasia. There are two forms of leukaemia. a. Myeloid leukaemia; or mylogenous leukaemia. b. Lymphatic leukaemia; or lymphogenousleukaemia. MYELOID LEUKAEMIA. In myeloid leukaemia the myeloid tissues are principally involved and cell of the myeloid series predominate in the blood picture. A fairly large number of neutrophils and neutrophil myelocytesare seen in the marked blood film taken from such a case, although there may be increased in the number of other forms of leucocytes also. The fatty bone marrow is replaced by hyperplasia of myeloid cells,giving it a pinkish gray colour. The spleen is enlarged but there is no change in the lymphtic glands. The internal organs often show fatty changes and small haemorrhages are frequently present. LYMPHATIC LEUKAEMIA. It occurs in lymphoid tissue of lymphocytic and their precursorin blood film in which lymphocytes may number more than 95 percent of the cells present. Lymphoblasts may become more numerousin very acute con dition, the red corpuscles sometimes show evidence of anaemia. In lymphatic leukaemia the most preominant changes are in the lymphatic glands,these being invariably enlarged.The spleen is also enlarged. Changes are also present in the bone - marrow, the normal cells being replaced by lymphocytes. Lymphocytic infiltration is often in the liver,kidney and other organs. The organs may be uniformally enlarged and palerthan normal or well defined tumour like swellings may be present. Internal organs may show degenerative changesof fatty nature and petechial haemorrhagesmay be present on the serious membranes. SPLENITIS. Inflammatory swelling of the spleen is seen in anthrax,anaplasmosis of cattle and acute infectious anaemia of horses.
- 18. Page 18 Macroscopically the spleen is enlarged and soft and its cut surface is dark red black,and the parenchyma is so soft that it may flow. MICROSCOPICALLY. There is marked hyperaemia, with collection of neutraphils, lympocytes, plasma cells and swelling is finally disintegration of the reticulum. CHRONIC SPLENITIS. May be characterized, either by induration (increase in the reticulum)or by cellular hyperplasia (increase in the parenchyma). The interstitial form of chronic splenitis is rarely seen in animals. Chronic splenitis in which pulp is increased is also uncommon. Specific infectious diseases,which supply good example of it are piroplasmosis of dogs infections anaemia of horses. In both diseases spleen is enlarged. In equine infectious anaemia the splenomegaly is due to increase in the size of the splenic nodules. The hyperplasia of the nodules is interpreted to be an attempt to increase antibody production. SUPPURATIVE SPLENITIS MAYARISE DUE TO. 1. As a result of septic emboli originating from mitral endocarditis or a result of metastatic lesion of pyogenic bacteria from more distant localized suppurative processes. In horses it occursin connection with strangles. 2. By penetration of infected sharp foreign bodies from the reticulum in cattle.