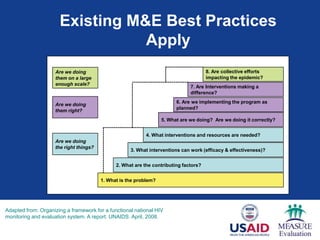
The document outlines a systematic approach to monitoring and evaluating integrated health interventions within health systems, emphasizing client-centered integration to enhance health outcomes. It details key steps and frameworks for effective implementation, including defining essential service packages, improving health information systems, and utilizing data for decision-making. The conclusions highlight the necessity of strong health systems and the role of leadership in guiding integration efforts while acknowledging the contextual nature of healthcare delivery.






















































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)