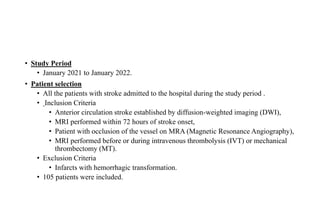
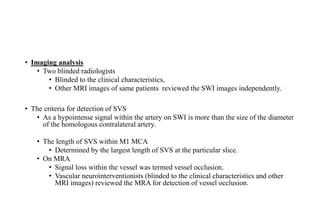
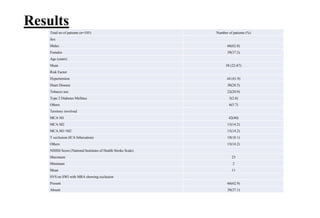
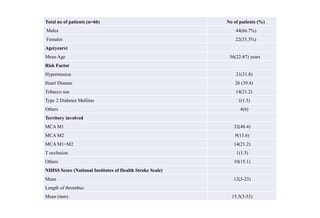
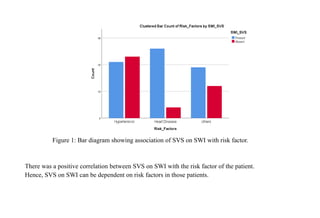
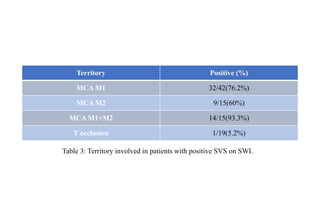
This study investigated the use of susceptibility vessel sign (SVS) on susceptibility weighted imaging (SWI) MRI to detect thrombus in patients with acute ischemic stroke. The study found that SVS was present in 62.8% of patients with confirmed vessel occlusion on MR angiography. SVS detection was correlated with risk factors like cardiac disease and territories of occlusion like the MCA. A moderate correlation was also found between thrombus length seen with SVS and NIH stroke scale scores. However, the study was limited by its small sample size and retrospective design. In conclusion, SVS on SWI can help identify thrombus location and burden in acute stroke.























![Case Discussion of Mechanical Thrombectomy[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casediscussionofmechanicalthrombectomy1-240303165457-27d0336d-thumbnail.jpg?width=640&height=640&fit=bounds)





































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)