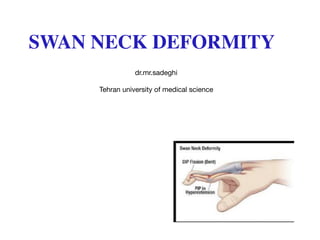
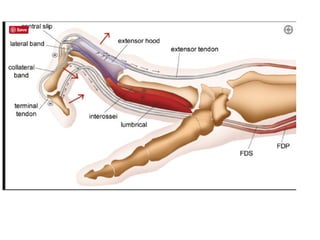
This document discusses swan neck deformity, which begins as a mallet deformity from extensor tendon disruption in the distal finger joint, causing overpull of the central slip and hyperextension of the proximal interphalangeal joint. This tightens the lateral bands and central tendon in a fixed dorsal position, preventing sliding over the condyles during flexion. There are three types of swan neck deformities - type I is flexible, type II requires intrinsic release in addition to procedures like dermodesis or tendon reconstruction due to intrinsic muscle tightness, and type III deformities are stiff and may require joint manipulation and skin/band mobilization even without significant joint destruction.















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
