Downloaded 126 times
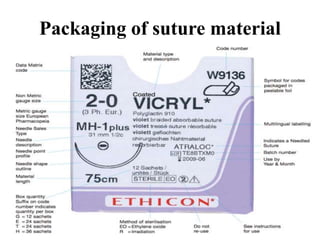
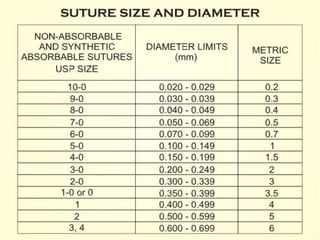
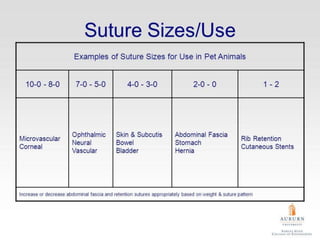
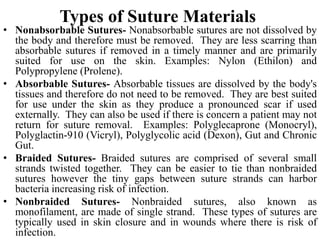
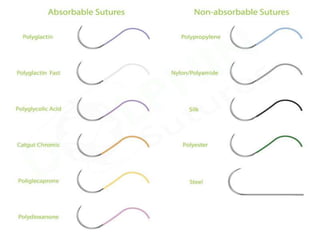
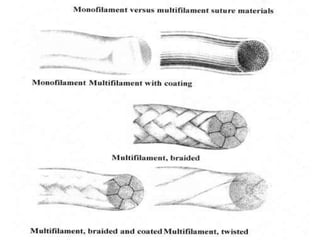
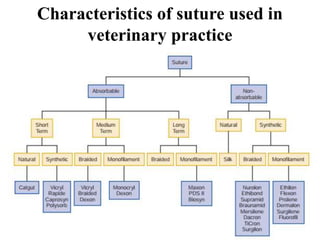
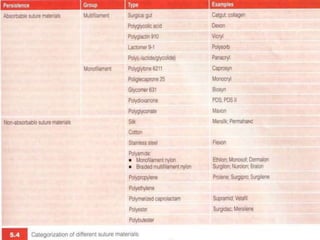
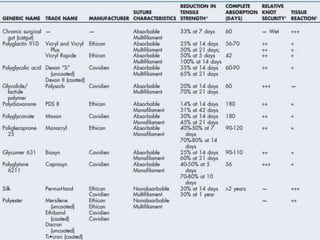
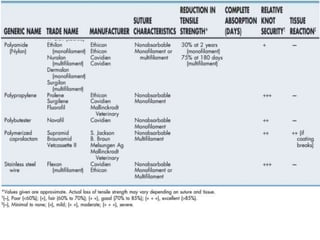
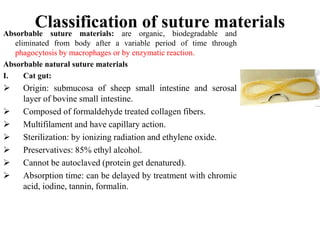

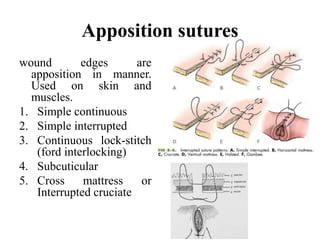
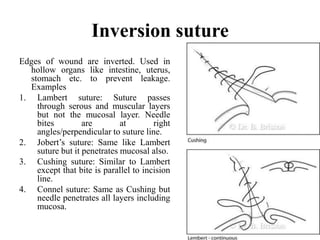
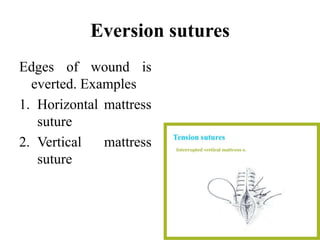
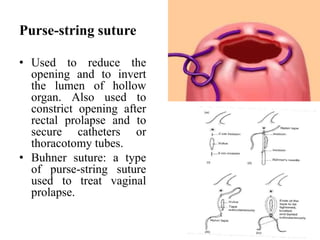


This document discusses sutures, suture materials, and suturing patterns used in veterinary practice. It covers the following key points in 3 sentences: Sutures are threads used to unite wound edges and are made from absorbable materials like catgut, collagen and synthetic polymers, or non-absorbable materials like silk, cotton and synthetic polymers like nylon and polypropylene. The document describes characteristics of different suture materials and various suturing techniques including apposition, inversion, eversion, and purse-string sutures as well as factors to consider like tissue strength and wound condition when selecting sutures. Common absorbable sutures mentioned are catgut, collagen



































































