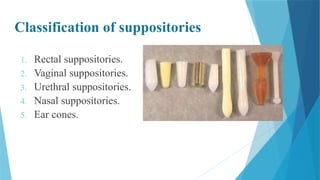
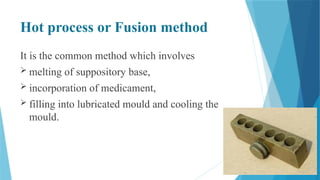
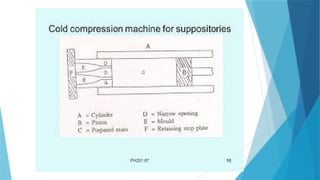
This document presents an overview of suppositories, highlighting their introduction, advantages, disadvantages, classifications, and preparation methods. It outlines various types of suppositories, including rectal, vaginal, urethral, nasal, and ear cones, detailing their characteristics and uses. Additionally, it discusses suppository bases, ideal properties, types of bases, and preparation methods such as hand rolling, hot process, and cold compression.
























































![IPL_PROJECT[1][1][1][1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/iplproject1111autosaved-250626172304-2bc65f41-thumbnail.jpg?width=640&height=640&fit=bounds)










![Tunnel_Diode[1].pdffdkjvnfvnfvkgvnjgrjvrgjbbjg](https://cdn.slidesharecdn.com/ss_thumbnails/tunneldiode1-241023150339-31eb82ff-thumbnail.jpg?width=640&height=640&fit=bounds)























