Downloaded 12 times



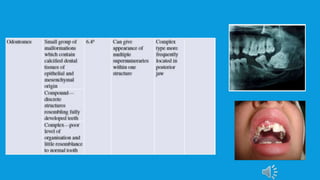


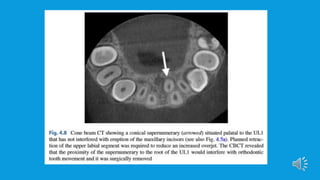

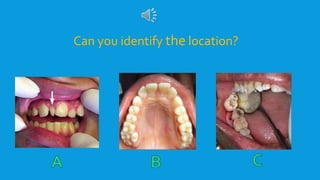


Supernumerary teeth are additional teeth that can develop in various locations in the dental arch, often leading to complications that may require removal. They are most commonly found in the permanent dentition and can occur in conjunction with syndromes, particularly in males. Management involves careful examination and imaging to determine the need for intervention, with treatment options based on the teeth's type, position, and effect on surrounding teeth.























































































